|
This article was previously published February 26, 2020, and has been updated with new information. Endocrine-disrupting chemicals (EDCs) are among the most destructive chemicals in our environment. Exposure to them is linked to growth, neurological and learning disabilities, obesity, diabetes, male and female reproductive dysfunction, birth defects, cardiovascular disease and some cancers.1 EDCs are not just harmful — they are also found almost everywhere and hard to avoid. They lurk in food packaging, nonorganic food, nonstick cookware,2 detergents, cosmetics,3 lotions, products with fragrance, antibacterial soaps,4 medicines, toys,5 fabrics, carpets, furniture, construction materials treated with flame retardants, pesticides and more.6 When an endocrine-disrupting chemical exerts permanent and even transgenerational changes to fat cells it is sometimes called an obesogen. Experts believe obesogens encourage the growth of fat cells and fat accumulation through metabolic and appetite alterations that increase the number and size of adipose cells. Examples of obesogens are bisphenol-A and parabens, and other obesogens may be found in flame retardants, pesticides and other chemicals. But the good news is there are at least five ways you can reduce your exposure to EDCs and obesogens, according to Dr. Leonardo Trasande, who wrote about EDCs for Medscape. Top Five Tips to Avoid Dangerous ChemicalsHere are my five tips, adapted from Trasande's article: 1. Beware of certain cookware -- Nonstick pans contain perfluoroalkyl substances, or PFAS, chemicals that slow the metabolism rate and cause weight regain.7 Cast iron and stainless steel cookware are good alternatives. Use glass to store your food and reusable storage bags at home and to bring food home from the grocery store. 2. Fight indoor pollution -- Flame retardants used in mattresses, carpets, furniture and electronics accumulate in household dust, impairing thyroid function. Open windows and use a wet mop to diminish them. Check if your upholstery has added flame retardants.8 3. Eat organic and avoid canned foods -- Organic food is free from GMOs and pesticides, which may disrupt the thyroid, impair cognition and cause cancer.9 Choose grass fed, humanely raised meat and dairy products. Canned foods may contain bisphenols, which are estrogenic and make fat cells larger. They persist in the environment, double Type 2 diabetes risk and likely pose toxicity to embryos.10 Don't use pesticides on your lawn, and remove shoes when you enter your house. 4. Don't microwave, and avoid packaged goods -- A "microwave safe" label is misleading because microscopic polymers break down and get into food.11 Processed and packaged foods contain high fructose corn syrup, artificial sweeteners, pesticides and other obesogens. Phthalates in food packaging and take-out containers can impair lipid and carbohydrate metabolism and increase weight.12 5. Avoid vinyl and plastic -- Use a cloth shower curtain that can be machine washed. These stay cleaner and last longer than vinyl. Replace luggage and backpacks with products made of organic blend canvas. Obesogens and Obesity Are LinkedObesity has become a worldwide epidemic. Between 1980 and 2010 the rate of obesity in the U.S. doubled and, worldwide, the rate of obesity tripled.13 Obesity in children is especially booming, almost always condemning them to life as obese adults.14 Obesity, because of its association with Type 2 diabetes, cancer and cardiovascular disease, costs the U.S. approximately $200 billion a year. The common belief that increased caloric consumption and reduced exercise cause the obesity epidemic does not explain the phenomenon, says research in the journal Basic & Clinical Pharmacology & Toxicology. Rather, people may be predisposed to obesity from exposure to obesogens in the womb, write the researchers.15
Other chemicals have similar effects, write the researchers, such as the fungicides triflumizole and tolylfluanid and the plasticizer diethylhexyl phthalate.16 Obesogens do not just increase the fat levels immediately seen in test animals: The fat augmentation properties may persist for generations, the researchers write.17
Apparently, obesogens not only can program organisms to accumulate fat; they can program their offspring to do the same. What Causes the Fat Accumulation to Occur?Researchers note in Basic & Clinical Pharmacology & Toxicology that cells exposed to an obesogen did not accumulate more fat than unexposed cells but differ in another way: they "did not respond to normal signalling processes." Specifically, write the researchers, the cells:18
Like the research in Basic & Clinical Pharmacology & Toxicology Research, a paper in Pediatric Research seems to confirm that obesogenic effects are seen transgenerationally. Fetal exposure to phthalates, which are obesogenic, is correlated with obesity in the exposed children, write the researchers.19
There Are More Obesity Links to ObesogensPerfluoroalkyl substances, or PFASs, which are endocrine-disrupting chemicals that are obesogenic, have also been linked to obesity in the scientific literature. A 2018 study in PLOS Medicine found:20
A 2018 study in Environmental Research on the exposure of pregnant women to phthalates also concluded:21
Endocrine Disrupting Chemicals Linked to DiabetesDiabetes is a major public health concern in the U.S. and other countries and endocrine disrupting chemicals contribute to the problem. Research in the journal Environmental Health Perspective finds "positive associations between exposure to BPA and BPS and the incidence of Type 2 diabetes, independent of traditional diabetes risk factors."22 Bisphenol A (BPA) and bisphenol S (BPS) are common EDCs. BPA is found in polycarbonate plastic and many canned foods, and metal jar lids have BPA in their linings.23 BPS, a BPA analogue, was thought to be safer than BPA, but research now reveals the two have similar risk profiles.24 Researchers in Environmental Health Perspectives wrote:25
Research in rats that was published in Environmental Health Perspectives in 2017 apparently duplicates the EDC and diabetes findings.26
The Endocrine Society Also Questions EDC SafetyThe Endocrine Society, the world's largest organization of endocrine clinicians and scientists, has also researched the risks of endocrine disrupting chemicals. The society says it:27
Toxic Chemicals Are EverywhereToxic chemicals are all around; in your food, water, air and countless commonly used products and goods, and this onslaught is having a definitive effect — even when exposures are relatively low. Yes, plastics have made modern life more "convenient" but the harm they cause is not worth it. The dangers are especially pronounced during pregnancy and early infancy. The idea that chemicals affect your health should come as no surprise. What may be surprising is the extent of your exposure. Most of us go about our day, touching, eating, drinking and breathing with few concerns about what we're actually coming into contact with. As you saw above in the different scientific studies, the obesogenic effects of EDCs are especially clear, causing obesity and other metabolic problems. Obesity, in turn, is linked to other diseases like diabetes, high blood pressure and certain cancers.28 But the damage from EDCs and obesogens can be reduced through commonsense lifestyle choices. from http://articles.mercola.com/sites/articles/archive/2022/01/28/how-to-avoid-edcs.aspx
0 Comments
As reported in this short news clip, research evidence1 shows that probiotics may help reduce long-haul symptoms after COVID-19. Some people experience symptoms for weeks or months after a COVID-19 infection has resolved. When these symptoms persist for four weeks or more, they are known as long COVID, long-haul COVID, chronic COVID or long-haul syndrome. Many of the symptoms of long COVID can also mirror those that are caused by the COVID-19 genetic therapy injections. Although anyone can experience symptoms of long COVID, it is more frequently seen in people who have been sick enough to be hospitalized or in the ICU. According to Dr. Peter McCullough, board-certified internist and cardiologist, 50% of those who have been sick enough to be hospitalized will have symptoms of long COVID:2
Symptoms of long COVID include fatigue, shortness of breath, coughing, chest pain, joint pain, memory problems, loss of taste or smell and muscle pain or headache.3 The symptoms are the result of damage to the lungs, immune system, mitochondria, heart and nervous system. McCullough goes on to explain that after a severe case of COVID-19, blood clots and heart problems can happen for up to 90 days or more. Inflammation to the lining of the heart — pericarditis — and around the lining of the lungs — pleuritis — can also occur in long COVID. Data from a study4 published in November 2021 show the administration of probiotics can affect the gut microbiome, and subsequently help your body heal from the symptoms of long COVID. Data Show Probiotics Help Long-Haul COVID SymptomsRoughly 12 million people may suffer from long COVID symptoms, which a Swedish study found could potentially be alleviated after 14 days of probiotics.5 The study was published September 2021 in the journal Medicines.6 The researchers wanted to evaluate how effective probiotics might be in alleviating two of the symptoms of long COVID — muscle soreness and brain fog. They enrolled 200 patients who had complaints of muscle fatigue after COVID. One hundred participants received a placebo and 100 received a combination of ImmunoSEB (systemic enzyme complex) and ProbioSEB CSC3 (probiotic complex). The participants were tested at different time points from Day 1 to Day 14. The data showed that those treated with the supplements had 91% resolution of muscle fatigue by Day 14. There was also a greater reduction in mental fatigue scores as compared to those receiving the placebo. The researchers concluded:7
ABC News interviewed public health medical educator Dr. Shad Marvasti, who recommends using probiotic supplements with at least 10 strains of active cultures to help support the immune system.8 He noted fermented foods such as sauerkraut, miso, kimchi and tempeh would help populate your gut microbiome. He also mentions yogurt. However, I recommend that if you do use yogurt, it's homemade since the products sold in the grocery store are high in sugar, which is a nutrient that feeds harmful bacteria in the gut. Also, if you decide to eat fermented soy, to be sure it’s grown organically, as most soy in the U.S. is a GMO food that is contaminated with pesticides and herbicides. During data-gathering for the research, the scientists found other coronavirus infections, such as SARS, also triggered long-term symptoms. During follow-up, data showed 64% reported muscle fatigue at three months, 54% at six months and muscle fatigue at 12 months in 60% of those surveyed.9 Likewise, after the Middle East Respiratory Syndrome (MERS), 48% reported fatigue after 12 months. The researchers believe that the supplement regimen used on the participants reduced physical and mental fatigue and would be an effective early intervention. They suggest that while scientists continue to characterize long haul syndrome, these dietary supplements are added to clinical recommendations to help improve functional status and quality of life.10 Poor Gut Health May Predict Severe COVIDIn an unrelated study published in 2018, researchers performed a systematic review of 70 randomized placebo-controlled trials11 to evaluate how specific probiotics may benefit individuals who had irritable bowel syndrome or other gastrointestinal (GI) disturbances. The data from the review indicated that there were specific probiotics with beneficial effects on lower GI health conditions, such as irritable bowel syndrome. Knowledge that probiotics offer a distinct advantage to the immune system has prompted study into the relationship between gut health and COVID outcomes. The featured study was published in the same month and year as another paper12 that proposed the use of postbiotics in the treatment of post-COVID long-haul symptoms. The writers advocate postbiotics that may help alleviate the burden on the body from viral infections and they postulate there may be a role for “precision postbiotics” in preventive interventions. Postbiotic is an umbrella term for components of microbial fermentation.13 This can include short-chain fatty acids, functional proteins, metabolites and extracellular polysaccharides. Since the start of the pandemic, several studies have shown that patients with GI symptoms often have more severe disease. One review of more than 1,000 patient records was presented to the American College of Gastroenterology.14 The data showed those who presented at admission with GI symptoms and suspected COVID-19 infection had worse outcomes than those who did not have GI symptoms. After adjusting for comorbidities, demographics and other clinical symptoms, of 1,000 patients, 22.4% had at least one GI symptom, the most common of which was nausea and vomiting. Researchers also found those who had GI symptoms had a higher body mass index, a higher prevalence of diabetes and high blood pressure, and were older. While this group had a higher rate of ICU admission and intubation, the study did not include mortality rates in the analysis. However, SciTech Daily15 reported that autopsy results and studies have suggested a sizable number of people with severe COVID-19 also have GI problems. A significant number of people with respiratory problems also had GI symptoms, suggesting that when the virus affects the GI tract, it can increase the severity of the illness. Another paper16 published in January 2021 suggested the GI symptoms that predict severe COVID-19 are triggered by poor gut health. The writer, Heenam Stanley Kim, Ph.D., from Korea University, proposes that gut dysbiosis can exacerbate the severity of the infection. This hypothesis is supported by a review of several studies since the start of the pandemic, which also demonstrated an association between severe disease and a lack of microbial diversity.17 An early study of patients admitted from March 4, 2020, to March 24, 2020, showed 31.9% had GI symptoms on admission.18 Your Gut Affects Brain Health and ImmunityYour gut health plays an important role in your neurological health and with your immune system. A very large part of your immune system sits in your gut microbiome and GI tract. Researchers estimate that up to 80% of your immune cells can be found in the gut.19 The complex interaction between your gut microbiome, pathogens and your immune system is affected by several factors, including your nutrition. One review of the research20 published in 2021 identified the significance that nutrition plays in both prevention and treatment of infectious disease. There are also deep connections that exist between your gut and your brain. Harvard Health21 explains that these two structures are linked through biochemical signaling. The primary connection is the vagus nerve, which is the longest nerve in the body. For example, when the fight-or-flight response is triggered, warning signals are sent to the gut. This is why digestive problems can be triggered by a stressful event. On the other hand, digestive issues like irritable bowel syndrome or chronic constipation can trigger anxiety or depression. Alzheimer's disease continues to be a leading cause of death in the U.S., with 1 in 3 seniors dying with Alzheimer's or dementia — more than the number killed by breast and prostate cancers combined.22 One team of Swiss and Italian researchers found a connection between imbalanced gut microbiota and the development of amyloid plaques in the brain, associated with Alzheimer's disease.23 In a prior study24 the team had found that the gut microbiota in people with Alzheimer's disease is different from those without the condition; microbial diversity is reduced, and certain bacteria are overrepresented. In their current study, the researchers engaged 89 people aged 65 to 85 years. Some were diagnosed with Alzheimer's disease or other neurodegenerative diseases and the others were healthy with no memory problems. The researchers used PET imaging to measure amyloid deposits in the brain and measure the serum markers of inflammation and proteins produced by intestinal bacteria. "Our results are indisputable: Certain bacterial products of the intestinal microbiota are correlated with the quantity of amyloid plaques in the brain," explained Moira Marizzoni, one study author with the Fatebenefratelli Center in Brescia, Italy.25 The Effects of Artificial Sweeteners, Sleep and SunlightSeveral factors influence your gut microbiome. One factor found in many processed foods that has a devastating effect on your gut microbiome is artificial sweeteners. As early as 2008,26 scientists had discovered that sucralose lowered your gut bacteria count by 47.4% to 79.7% and increased the pH level of your intestines. More recently, scientists found that three of the most popular artificial sweeteners — sucralose (Splenda), aspartame (NutraSweet, Equal and Sugar Twin) and saccharin (Sweet’n Low, Necta Sweet and Sweet Twin) — have a pathogenic effect on two types of gut bacteria.27 Lab data demonstrated the products can trigger beneficial bacteria to become pathogenic and potentially increase your risk of serious health conditions. This was the first study to demonstrate how two types of beneficial bacteria can become diseased and invade the gut wall. The bacteria studied were Escherichia coli (E. coli) and Enterococcus faecalis (E. faecalis). This research supports past evidence that noncaloric artificial sweeteners induced “compositional and functional alterations” in the gut microbiome.28 Data have also shown that artificial sweeteners can increase the permeability of the intestinal epithelial barrier, which leads to systemic inflammatory diseases. In the lab,29 high concentrations of aspartame and saccharin induced cell death and at low concentrations, it increased the epithelial permeability. Two strategies that also play a role in your gut microbiome are getting more sleep and sunshine. Researchers have found a curious bidirectional link between your gut health and sleep. One study published in the Frontiers of Psychiatry noted:30
As noted in the Frontiers in Psychiatry study,31 mounting research suggests your gut microbiome helps regulate not only your mood but also your sleep cycle through what's known as the gut-brain axis — a bidirectional communication "highway" that links your central and enteric nervous systems.32 During the past pandemic months, it has become increasingly obvious that maintaining optimal levels of vitamin D could help reduce your risk of infectious disease.33 A research team from the University of British Columbia was also interested in how exposure to UVB light may affect the human gut microbiome.34 Past studies had suggested vitamin D could alter the gut microbiome35 and since there are few natural foods that contain vitamin D,36 a vast majority of your body's requirement is usually met through skin exposure to UVB light.37 The researchers from British Columbia noted that past research has shown sunlight has a positive effect on those with inflammatory bowel disease and multiple sclerosis, both of which are exacerbated by inflammation.38 In this clinical pilot study the researchers found the fecal microbiota were positively altered after exposure to sunshine. They wrote:39
Optimize Your Gut MicrobiomeThe choices you make every day have an impact on your gut microbiome. Optimizing your gut flora and vitamin D level is crucial to good health. Regularly eating traditionally fermented and cultured foods is the easiest, most effective and least expensive way to make a significant impact on your gut microbiome. Healthy choices include lassi (an Indian yogurt drink), cultured grass-fed organic milk products such as kefir and yogurt, natto (fermented soy) and fermented vegetables of all kinds. Generally, I believe the majority of your nutrients need to come from food. However, supplemental probiotics are an exception if you don't eat fermented food on a regular basis. Spore-based probiotics, or sporebiotics, can be helpful if antibiotics are necessary. In addition to getting enough quality sleep and maintaining optimal levels of vitamin D, it is also important to feed your beneficial bacteria the nutrients they need to thrive. While harmful bacteria thrive on sugar and carbohydrates, beneficial bacteria thrive on fiber. According to a study published in 2019 in The Lancet40 people eating 25 to 29 grams of fiber each day had a reduced risk of a range of critical outcomes, such as stroke, coronary heart disease, Type 2 diabetes and all-cause mortality. However, they found eating 29 grams a day was merely adequate, writing:41
from http://articles.mercola.com/sites/articles/archive/2022/01/28/probiotics-improve-long-covid.aspx What you eat plays a significant role in how well your immune system functions. As a result, you can actively support your body’s ability to ward off acute and chronic conditions with each food you put into your mouth. However, depending on your food choices, you can also hinder it. What’s the worst ingredient for your immune system? If you guessed sugar, nice try, but there’s an even worse offender that’s just as prevalent but not as widely recognized for its pernicious influence on health: industrially processed seed oils, often referred to as “vegetable oils.” At the root of the harmful biochemical reactions triggered by seed oils is linoleic acid, which is an 18-carbon omega-6 fat. Linoleic acid is the primary fatty acid found in polyunsaturated fatty acids (PUFAs) and accounts for about 80% of the fatty acid composition of vegetable oils. Omega-6 fats must be balanced with omega-3 fats in order to not be harmful, but this isn’t the case for most Americans. Why Seed Oils Are Even Worse Than SugarAn immunologist with CNBC News recently named sugar the “worst food ingredient for your immune system,”1 in large part because consuming too much of it can contribute to insulin resistance and obesity, which increases inflammation in your body and causes damage to blood vessels. While your immune system is busy tending to these areas, CNBC notes, “This creates a major distraction for the immune system and paves the way for dangerous bacteria and viruses to slip through our body’s defenses.”2 In fact, it’s been known since at least the 1970s that sugar weakens the immune system (while fasting strengthens it),3 and I recommend limiting added sugars to a maximum of 25 grams per day or 15 grams a day if you're insulin resistant or diabetic. But most health “experts” simply do not understand that seed oils are even worse than sugar. These fats become embedded in your cell membranes and stay there for about seven years, wreaking havoc on your health. Not only are most of the omega-6s you eat, including seed oils, damaged and oxidized through processing, but even if they are unheated and pristine when consumed in any but small amounts, your body degrades them into free radicals that damage virtually every tissue in your body. "Most of this linoleic acid, when it oxidizes, it develops lipid hydroperoxides and then these rapidly degenerate into … oxidized linoleic acid metabolites," says Dr. Chris Knobbe, an ophthalmologist and the founder and president of the Cure AMD Foundation.4 OXLAMs (oxidized linoleic acid metabolites) create a perfect storm, as they are cytotoxic, genotoxic, mutagenic, carcinogenic, atherogenic and thrombogenic, according to Knobbe. Their atherosclerosis and thrombogenic actions are especially concerning because they can produce strokes and clots, however metabolic dysfunction can also occur. During the lipid peroxidation cascade caused by the excess consumption of omega-6 seed oils, PUFAs accumulate in your cell membranes, leading to a peroxidation reaction. Because there are so many reactive oxygen species it leads to the development of insulin resistance at the cellular level. OXLAMs are also toxic to the liver and are associated with inflammation, fibrosis and fatty liver disease in humans.5 Dr. Paul Saladino, a physician journalist, also explained in a podcast that linoleic acid "breaks the sensitivity for insulin at the level of your fat cells,”6 essentially making them more insulin sensitive — and, since your fat cells control the insulin sensitivity of the rest of your body by releasing free fatty acids, you end up with insulin resistance. Linoleic Acid Drives Chronic Diseases, Worsens COVID-19There’s virtually nothing more destructive to your body than seed oils in producing heart disease, cancer, age-related macular degeneration, diabetes, obesity and dementia.7 When I interviewed Tucker Goodrich, who developed an IT risk management system used by two of the largest hedge funds in the world, then transitioned into medical research, he explained that animals typically develop cancer once the linoleic acid in their diet reaches 4% to 10% of their energy intake. Yet, most Americans get approximately 8% of their calories from seed oils. "So, we're way over what these thresholds in the lab would suggest is a safe level of these fats based on the laboratory work in animals," Goodrich said, adding:
Data also indicate that COVID-19 mortality rates are heavily influenced by the amount of unsaturated fats you eat. Simply put, unsaturated fat intake is associated with increased mortality from COVID-19, while saturated fat intake lowers your risk of death.8 The authors noted that unsaturated fats "cause injury [and] organ failure resembling COVID-19." More specifically, unsaturated fats are known to trigger lipotoxic acute pancreatitis, and the sepsis and multisystem organ failure seen in severe cases of COVID-19 greatly resembles this condition. In short, linoleic acid contributes to the inflammatory domino effect that eventually kills some people with COVID-19. Goodrich explained:
It's Hidden in ‘Healthy’ Foods, Like Chicken and Olive OilAnother reason why linoleic acid is so harmful is because it’s found in virtually every processed food, including restaurant foods, sauces and salad dressings. Many processed foods high in sugar also contain seed oils, which is why eliminating them from your diet is essential for improving and maintaining your health. However, even if you cut out processed foods and skip sauces and salad dressings when you eat out, you may still be consuming too much seed oil because it’s hidden in “healthy” foods like chicken and pork. The problem is that these animals are fed grains that are high in linoleic acid,9 which makes the meat a major source as well. So if you’re eating chicken and pork, believing it to be good for you, you’re being misled. Olive oil is another health food that’s a hidden source of linoleic acid; however, there are caveats. As Goodrich explained, the linoleic acid content of olive oil can vary significantly. "The percentages that I've seen quoted in literature range from 2%, which is awesome, to 22%, which is not good," he said. Olive oil also has the benefit of containing beneficial oleic acid, which is protective against both cardiolipin oxidation and LDL oxidation. Cardiolipin is a type of fat located in your mitochondria, and oxidation of cardiolipin is one of the things that controls autophagy. By altering the composition of cardiolipin in your mitochondria to one that's richer in omega-6 fats, you make it far more susceptible to oxidative damage. Goodrich cites research showing that when the linoleic acid in cardiolipin is replaced with oleic acid like that found in olive oil, the cardiolipin molecules become highly resistant to oxidative damage. The other variable, however, is that olive oil is often cut with cheaper seed oils, which raises the linoleic acid content. So if you consume olive oil, I strongly recommend keeping close track of your total linoleic acid intake. How Much Linoleic Acid Is Too Much?Many now understand that your omega-6 to omega-3 ratio is very important, and should be about 1-to-1 or possibly up to 4-to-1, but simply increasing your omega-3 intake won't counteract the damage done by excessive linoleic acid. You really need to minimize the omega-6 to prevent damage from taking place. Ideally, consider cutting linoleic acid down to 2 or 3 grams per day, which is close to what our ancestors used to get before all of these chronic health conditions, including obesity, diabetes, heart disease and cancer, became widespread. If olive oil puts you over the limit, consider cooking with tallow or lard instead. Beef tallow is 46% oleic acid and lard is 36% oleic acid. Remember, linoleic acid is considered an essential fat, so you don’t want to eliminate it entirely. It’s only when consumed in excessive amounts that linoleic acid acts as a metabolic poison — but virtually everyone is consuming excessive amounts. What amount is “excessive”? Anything over 10 grams a day is likely to be problematic, although the exact cutoff is still unknown. In 1909, Americans ate 2 grams a day of vegetable oil, according to Knobbe, but by 2010 this had increased to 80 grams a day.10 If you’re not sure how much you’re eating, enter your food intake into Cronometer — a free online nutrition tracker — and it will provide you with your total linoleic acid intake. The key to accurate entry is to carefully weigh your food with a digital kitchen scale so you can enter the weight of your food to the nearest gram. Cronometer will tell you how much omega-6 you're getting from your food down to the 10th of a gram, and you can assume 90% of that is linoleic acid. Again, anything over 10 grams is likely to cause problems. Since there's no downside to limiting your linoleic acid, you'll want to keep it as low as possible, which you do by avoiding high-LA foods. This means eliminating all of the following oils:
Other high-LA foods include chips fried in vegetable oil, commercial salad dressings and sauces, virtually all processed foods and any fried fast food, such as french fries. I'm currently writing a book on this topic as well, so stay tuned for more information about what I believe is likely the leading contributing cause of virtually all chronic diseases we've encountered over the last century. from http://articles.mercola.com/sites/articles/archive/2022/01/27/vegetable-oil-linoleic-acid.aspx As of January 7, 2022, just over a year into the campaign to inject every human being with a gene transfer product to protect against COVID, the U.S. Vaccine Adverse Events Reporting System (VAERS) has received 9,936 reports of death following the COVID jab in the United States’ territories alone.1 When you include foreign reports received by VAERS, the death toll stands at 21,745. A total of 1,541 miscarriages have also been reported post-jab in the U.S., or 3,594 if you include foreign reports. Despite these shocking statistics, U.S. health officials and “fact checkers” insist not a single death can be attributed to the shots. During an early January 2022 Senate committee hearing on the nation’s Omicron response (see video above), Centers for Disease Control and Prevention director Dr. Rochelle Walensky, and director for the National Institutes of Allergy and Infectious Diseases, Dr. Anthony Fauci, testified — under oath — that they “did not know” how many deaths had been reported to VAERS following COVID “vaccination.”2,3 Walensky referred to the shots as “incredibly safe,” claiming — against all science — that they “protect us against Omicron, they protect us against Delta, they protect us against COVID.” She also falsely claimed that all reported COVID-19 vaccine deaths have been “adjudicated.” No, VAERS Is Not a Repository of Fake ReportsWorse yet, both Walensky and Fauci claim any and all adverse events following vaccination get reported to VAERS, including accidental deaths and car accidents. They both actually claim that if a person gets the COVID shot and gets hit by a car afterward, that is reported as an adverse reaction. Nothing could be further from the truth. First of all, adverse events are not automatically reported and, certainly, obvious accidents are not entered into the system as a suspected vaccine side effect. As reported by Health Impact News,4 there are about 18 reports in VAERS that include “road traffic accident,” but most if not all relate to an adverse event, such as a heart attack, occurring while driving. They were not hit by someone else and entered into the system. As noted by Pam Long in a January 12, 2022, Twitter thread:5
VAERS was designed and created as an early warning system. It’s true that anyone can file a report, but it’s time-consuming, requires the knowledge of medical details a patient oftentimes won’t have, and carries penalties for filing a false report. There’s absolutely no reason to suspect, let alone assume, that people are filing false reports just to make the shots look bad. Fact Checker Outs Himself as a Pharma PropagandistWalensky and Fauci aren’t the only ones lying about the lethality of the COVID jab. Mainstream media are all-in as well. In a USA Today fact check,6 Daniel Funke claims that “COVID-19 vaccines [are] safe for children” and “not linked to deaths.”
Funke cites data from Pfizer’s clinical trials, “which found the vaccine was safe” for children, as “no deaths were reported” in Pfizer’s trials for 12- to 25-year-olds, and those for 12- to 17-year-olds. Funke dismisses the rationale for looking at VAERS data on the basis that anyone can file a report and that reports are unverified, and therefore cannot be used to determine causation. All Opinion and No DataThere are so many issues with this “fact-check,” no wonder Facebook attorneys are using the legal defense that fact checks are “opinion” only and not actual assertions of fact.7,8 There’s nothing but opinions in this piece. As “evidence” that the COVID shots are safe and have caused no deaths, Funke presents:
It’s hard to come up with a less compelling list of evidences for safety, but then again, propagandists have to work with what they have, and in this case, they have nothing. Funke presents zero actual data to support his opinion. Explain the Rise in Mortality if You CanThere are many data-driven reasons to suspect, predict and even assume that the COVID shots are killing more people than they’re saving — regardless of the age group in question. It would take an entire book to cover it all, so I will only review a few of those reasons here. One very telling clue that recently came to light is life insurance data. According to OneAmerica, a national life insurance company based in Indianapolis, in the third quarter of 2021, working-age Americans (aged 18 to 64) died at a rate that is 40% higher than the prepandemic rate, and they didn’t die from COVID.10 And, according to CEO Scott Davidson, this catastrophic abnormality is consistently seen “across every player” in the life insurance industry.11 A 40% increase in mortality is simply unheard of, and as of yet, they claim to have no clue as to what’s causing young and middle-aged people to die prematurely at such an astounding rate. Looking at it from a sleuth’s point of view, one might ask, “What environmental factor with unknown safety was introduced in 2021 to people in this age group?” Sure, pandemic restrictions have led to spikes in drug overdoses and suicides, which affects this cohort in particular. But “deaths of desperation” cannot account for all of it. The one wild card is the COVID jab. More than 173 million working-age Americans (18 to 64) got these experimental gene transfer injections,12 and doctors and scientists have elucidated several mechanisms by which they might injure or kill. What’s more, the rise in deaths began AFTER the rollout of the shots, and whatever the causative factor, it is not only national but likely international in scope. The Insurance Regulatory and Development Authority of India, for example, also reports a 41% rise in death claims in 2021.13 Excess deaths (exceeding prepandemic norms) are also reported in the U.K.14 Among teens (aged 15 to 19), mortality spiked right after teens became eligible for the COVID shot.15 Between the week ending June 26 and the week ending September 18, 2020, and that same period of time in 2021, teenage deaths rose by 47%.16 A rise in disability claims17 also suggests that many who aren’t killed by this novel lethal threat are seriously injured, often long-term. For all of these reasons, the COVID jabs cannot be taken off the table. Logic demands that they be looked into as a potential causative factor. Can VAERS Data Demonstrate Causality?One person who has taken a strong stance against the claim that VAERS data cannot tell us anything about causation is Steve Kirsch, executive director of the COVID-19 Early Treatment Fund. In the video “Vaccine Secrets: COVID Crisis,”18 he argues that VAERS can indeed be used to determine causality. It’s important to realize that the idea that VAERS cannot show causality is part of how and why the CDC can claim none of the deaths is attributable to the COVID shot. Kirsch argues that this premise is in fact false, and that causation can be determined using VAERS’ data. To prove his point, Kirsch gives the following analogy: Suppose you give a two-dose vaccine. After the first dose, nothing happens, but after the second dose, people die within 24 hours of a deep vein thrombosis (DVT). When you look at the VAERS data, what you would find is no reports associated with the first dose, and a rash of deaths after the second dose, all within the same timeframe and with the same cause of death. According to the CDC, you cannot ascribe any causality at all from that. To them, it’s just random chance that everyone died after the second dose, and from the same condition, and not the first dose or from another condition. Kirsch argues that causality can indeed be identified from this kind of data. It’s very difficult to come up with another explanation for why people — many who are young, in perfect health with no predisposing conditions — die exactly 24 hours after their second dose. It’s even difficult to come up with another explanation for people who do have underlying conditions. For example, is it reasonable to assume that people with, say, undiagnosed heart conditions, would die from DVT exactly 24 hours after getting a second dose of vaccine? Or that people with undiagnosed diabetes would die from DVT exactly 24 hours after their second dose? Why not after the first dose, or two months after the second dose, or any other random number of hours or days, or for other random cause of death? Why would people randomly die of the same condition at the exact same time, over and over again? At bare minimum, as an early warning system, VAERS is designed to flag potential causation. It’s by looking for repeated patterns of side effects that you would begin to identify a potentially problematic vaccine. Once a pattern is identified — and there’s no denying death within 24 hours to one week is a pattern seen for the COVID shots — an investigation should be launched. But no such investigation has been launched for the COVID jabs. Clear-cut patterns are simply ignored. As an early warning system, VAERS is performing as intended, despite severe underreporting (the CDC recently published a paper in which they admit COVID jab adverse effects in children are underreported by a factor of 6.519). It’s the follow-up that’s lacking. But lack of investigation and follow-up is not evidence that the shots can’t cause death. ‘Bad Batches’ Are Another ClueAnother clue that hints at SOME of the shots being able to cause rapid death is the “bad batch” phenomenon. Independent investigations have revealed that some lots of the shots are associated with very severe side effects and death, whereas other lots have no adverse events associated with their use. According to howbadismybatch.com, a site that matches up vaccine lot codes with reports in the VAERS system, approximately 5% of the lots are responsible for 90% of all adverse reactions. Some of these batches have 50 times the number of deaths and disabilities associated with them, compared to other lots.20 Another website that basically does the same thing is TheEagle’s VAERS Dashboard. (A video explaining how to use the dashboard can be found on Bitchute.21) Dr. Reiner Fuellmich, cofounder of the German Corona Investigative Committee, and Dr. Wolfgang Wodarg, a former member of the German parliament, discuss this “smoking gun” evidence in the video above. According to Fuellmich and Wodarg, this lot-dependent data shows vaccine makers are conducting secret experiments within the larger public trial. They appear to actually be doing lethal-dose testing on the public. Wodarg argues that the evidence for this is very clear from the data. They also appear to be coordinating these lethal-dose experiments, so that they’re not all releasing their most toxic lots at the same time, or in the same areas, so as to avoid detection through clustering. More Data Showing COVID Jabs Can KillIn closing, I will raise just two more pieces of evidence that speaks to COVID jabs having the ability to kill large numbers of people: • A recent histopathologic analysis of the organs from 15 patients who died within seven days to six months’ post-jab, ages 28 to 95, found 14 of the deaths — 93% — were caused by the jab.22,23 None of the original coroners’ reports implicated the shots, however. The association was only established through autopsy, which revealed a “process of immunological self-attack” that is “without precedent.” “Because vaccination was the single common denominator between all cases, there can be no doubt that it was the trigger of self-destruction in these deceased individuals,” Drs. Sucharit Bhakdi and Arne Burkhardt wrote. • According to researchers at Columbia University, the real number of people killed by the COVID jabs is about 20 times the reported rate, based on their analysis of two publicly available databases (VAERS in the U.S., and another in Europe).24,25,26 That analysis was published in October 2021, but few ever heard a peep about it. According to the authors:
Based on the ever-mounting data, the claim that COVID shots have not, cannot, and/or will not cause death simply isn’t credible. And the longer these shots continue to be used, the greater the likelihood that they will indeed kill far more than the actual virus ever did. We also need to remember that the disabilities and long-term chronic ill health these shots are causing will prematurely kill many more, even if it takes 10 or 15 years, and we have no data on any of that yet. from http://articles.mercola.com/sites/articles/archive/2022/01/27/health-officials-deny-death-from-covid-shots.aspx This article was previously published April 30, 2020, and has been updated with new information. You may know visceral fat by another name — belly fat. In fact, it goes by several names such as "beer belly" and "middle-age spread." While many see it as an aesthetic problem, carrying extra weight in your midsection has a significant effect on your physical health, including your brain. You have two basic types of fat. Subcutaneous fat is found just under the skin and is the type that jiggles and dimples. Visceral fat is found under the abdominal muscle, wrapped around your internal organs. This type is more dangerous as it's linked to the production inflammatory cytokines and is considered biologically active.1 Visceral fat also increases insulin resistance and your risk for metabolic syndrome. It plays a role in the development of Type 2 diabetes, heart disease, breast cancer, colorectal cancer and Alzheimer's disease.2 While many consider their body mass index (BMI) as an indication of whether they fall into a category of overweight or obesity, it is your waist measurement in combination with your waist-to-hip ratio that is a better indication of health. This measurement of visceral fat helps predict your potential risk for chronic disease and even mortality. Where fat deposits on your body has a distinct impact on your health. Deposits in the hips and thighs result in a pear shape that has a lower potential risk for chronic disease than those with fat deposits in the abdomen, described as an apple shape. Visceral Fat Associated With DementiaOne of the first studies3 in which researchers evaluated the association between belly fat and dementia was published in 2008. An analysis was conducted of 6,583 people in Northern California. Abdominal measurements were taken and 36 years later researchers looked for recorded diagnoses of dementia in the participants. Of the cohort, 15.9% were diagnosed with dementia. Researchers compared those with lowest abdominal girth against the highest and found the highest had a three-fold increased risk. In the past decade the terms "normal weight metabolic obesity," "skinny fat" and "normal weight obesity" have been used to describe those who have a normal BMI but have metabolic characteristics of being obese.4 These individuals carry excess belly fat. One of the risks associated with a high waist-to-hip ratio, even when having a normal weight, is declining cognitive function. But not all studies yield straightforward results linking the two conditions. In a cross-sectional autopsy study,5 researchers evaluated 234 participants with abdominal visceral fat measured on autopsy. They looked for associations between visceral fat and cognitive impairment as defined by clinical dementia. What they found were those who had higher amounts of central obesity had a lower risk of dementia later in life. Although the authors of other studies found a relationship between obesity and cognitive impairment, the researchers expected those findings since the measurements were made at the same time and the samples were mainly of older adults. In past studies scientists have demonstrated a link between obesity and a higher risk of cognitive function decline, yet when measured later in life the results are conflicting. The researchers reported on several studies that used a direct measurement of abdominal visceral fat and had demonstrated the same relationship found in this study. In one, a significant reduction in BMI later in life increased the risk of developing dementia in the following three years by 118%. Study Finds a Pathway That Visceral Fat Affects CognitionIt's not enough to know a link exists. Scientists also want to know what happens at a molecular level. Researchers from Augusta University recently published a study6 that showed, for the first time, one pathway visceral fat may use as it damages your brain cells. The effect influences the microglia, or immune cells in the brain, to change behavior and then trigger functional damage to your neurons.7 The results are important, as one of the researchers commented in a press release from the University:8
The signal is a proinflammatory protein called interleukin-1 beta that doesn't often enter the brain. However, visceral fat "generates high, chronic levels of the signal that in turn over-activate the usually protective microglia, the resident immune cells in our brain." Research has demonstrated these reactions were problematic and this offers evidence as to how they are triggering problems. Using an animal model, the researchers studied the effect on cognitive function and inflammation.These findings help to add pieces to the puzzle of how interleukin-1 beta may affect actions in the central nervous system. Bigger Belly Predicts Heart Disease Better Than BMIAfter a lifetime of exposure to pathogens and toxins, a weakened and overactive immune system may trigger chronic inflammation.9 When the inflammatory response triggered by visceral fat is added to this burden it may be a better predictor of heart health than your overall weight. This means those who are normal weight with visceral fat carry a greater risk than they may imagine. Two studies that were released almost simultaneously revealed similar results — those who carry a spare tire have a greater risk of heart failure or heart disease. The first from the Norwegian University of Science and Technology was a meta-analysis of 23 studies with 650,000 participants. They looked at BMI and the risk of heart failure, finding the risk rose 41% with a rise of five BMI units and accelerated with greater weight gain.10 Those who were obese had a risk two to three times greater than their normal weight counterparts. The researchers also noted for every 10 centimeters (approximately 4 inches) of an increase in a participant's waist measurement, there was a 29% increased risk of heart failure. The leaders of several of the studies had adjusted for factors that affect heart health, such as high blood pressure, diabetes and a poor lipid profile, but those with a higher waist circumference continued to have a greater correlation. One of the scientists from the study commented:
The second study from the Intermountain Medical Center Heart Institute and Johns Hopkins Hospital evaluated the risks of central obesity as a predictor of heart disease in those also suffering Type 1 or Type 2 diabetes without previous symptoms of heart disease.11 The team started with 200 participants who met the criteria and discovered that independent of total body weight, central obesity "was strongly associated with regional left ventricular dysfunction, which is a common cause of heart disease, including congestive heart failure." The results were presented at the 2016 American College of Cardiology Scientific Session. The co-director of research from Intermountain Medical Center Heart Institute, Dr. Brent Muhlestein, commented on the results of the study and the implications it has on assessment and treatment.12
Stomach Fat Affects Mental HealthVisceral adipose tissue is also linked to mental health conditions such as depression and anxiety. In one study of postmenopausal women, those with abdominal obesity were more likely to struggle with depression than those without. This led the researchers to conclude that "visceral fat accumulation was an independent and positive factor significantly associated with the presence of depressive symptoms."13 Men also suffer from a higher risk of depression with abdominal obesity, as demonstrated by a study of 2,502 men and women. The researchers measured leptin levels and visceral fat and used either an assessment scale or antidepressant prescription to measure depression.14 They found higher levels of leptin increased the risk of depression in men, leading this team to conclude:
The link between abdominal obesity and depression may be related to the inflammatory response the active fat triggers. Inflammation has a link to depression as demonstrated in several studies. In a literature review15 of 30 studies with 1,610 participants, researchers found anti-inflammatory agents reduced symptoms of depression when compared to a placebo. These results support other evidence finding a link between inflammation and depression.16,17 Unfortunately, mental health screening may overlook this factor. Evaluate Your Risk With Waist-to-Hip RatioAs demonstrated in this short video, using a waist-to-hip ratio is a more reliable indication of your future risk of chronic disease, heart disease and mental health. A higher ratio is suggestive of more visceral fat accumulation around your abdominal organs, which is far more hazardous to your health than the subcutaneous fat located directly under your skin. To determine your waist-to-hip ratio you'll want to measure both areas. Start by measuring your waist using a spring-loaded or cloth tape measure. Find your waist, which is your midpoint between your last rib and your iliac crest. These are the bones on the front of your abdomen, as shown in this video. Measure the area in the middle without pulling the tape measure too tight. Take a couple of measurements, allowing 30 seconds between each one to allow your skin and subcutaneous tissue to return to normal. Be sure to take the measurement at the same place each time. Using just your waist circumference, your risk categories are:
Your hip measurement is taken at the widest part of your buttocks, again without pulling the tape too tightly and taking at least two measurements for accuracy. You get your ratio by dividing your waist measurement by your hip measurement. These are the waist-to-hip ratio norms:
Approaches to Addressing Belly FatAs I've written before, doing spot reducing exercises won't burn through subcutaneous or abdominal fat. You may build strong core muscles, but they'll still be hidden under subcutaneous fat. People use the term "spot reduction" to refer to the idea you can affect layers of fat in one area of the body by exercising muscles in that area. Visceral fat is more dangerous than subcutaneous fat but is also easier to gain and to lose. Along with practicing intermittent fasting and eating a ketogenic diet to support your mitochondrial health and weight loss efforts, these strategies may help you lose both subcutaneous and visceral fat: • Reduce stress -- Located on top of each kidney are your adrenal glands. Cortisol is a steroid produced by these glands related to your "fight or flight" response. When you're under chronic stress cortisol increases fat distribution to your abdominal area.18 • Stay hydrated -- Drinking water may be one of the easiest ways to reduce psychological and physical stress. Your body is made of more than 60% fluid and your kidneys require fluids to flush toxins from your body. When you're dehydrated it affects the release of cortisol and alters metabolism.19 You'll know you're well hydrated by the color of your urine, which should be light straw-colored. • Quality sleep -- Maintaining adequate amounts of quality sleep will help you control stress. Loss of sleep may alter your production of hormones, including cortisol, and leave you vulnerable to the effects of daily stress. Sleep deprivation may lead to an increase in cortisol20 leading to a compromised immune system and disruption in metabolism and cognitive impairment. • Control insulin level -- Your body produces insulin in response to eating carbohydrates, which works with cortisol to help regulate your blood sugar levels.21 By reducing your carbohydrate intake you'll reduce your insulin secretion and may help reduce the accumulation of visceral fat. • Optimize vitamin C -- Vitamin C offers resilience against stress22 and plays a role in stabilizing blood sugar, which contributes to the production and release of cortisol. When you eat multiple servings of vegetables and fruit each day, you help maintain your levels of vitamin C. Remember, fresher produce tends to have higher concentrations of vitamins. from http://articles.mercola.com/sites/articles/archive/2022/01/27/effects-of-visceral-fats.aspx Vaccine passports are poised to change the world as you know it, creating a digital trail of your every move. Right now, it’s injection status that’s being highlighted, but the end goal is to surveil and collect not only medical information but financial transactions, political affiliations, religious and philosophical beliefs and more. Some have speculated that the introduction of digital IDs and vaccine passports in the U.S. is laying the infrastructure for a social credit system. China’s social credit system, a massive undertaking of government surveillance that aims to combine 600 million surveillance cameras — about one for every two citizens — with facial recognition technology, has the reported goal of being able to identify anyone, anywhere, within three seconds.1 It’s difficult to imagine this type of tyranny transpiring in the U.S. — until you look back over the last two years. In 2019, it may also have seemed farfetched that you’d have to receive an injection of an experimental gene therapy in order to enter certain restaurants, gyms, entertainment venues and workplaces, yet, here we are. As investigative journalist Corey Lynn, who recently detailed not only why it’s so important to stop vaccine passports but also 22 practical ways to do so, put it:2
Are We Being Trained Like Dogs?Lynn compared the vaccine ID passport system being rolled out to mandatory rabies vaccines for dogs. It might seem like a stretch, but there are many similarities between the rabies vaccine system and what could soon happen on a global scale, but this time to people, not dogs. Lynn writes:3
Your dog can’t visit doggy day cares, dog parks or grooming centers unless he’s received the rabies shot. Failure to comply leaves your dog ostracized and you, as its owner, vulnerable to fines. Lynn argues that, much like COVID-19, millions of pet owners have blindly gone along with the required rabies vaccines for their pets, despite questions over its safety and necessity on an annual basis, as studies suggest the shots may provide protection for more than six years.4 “They have tested this system on pet owners for years, and half the U.S. population willingly went along with this without even questioning it. Sound familiar?” Lynn asks. “… They are treating you like a dog, and they didn’t even show dogs the respect they deserve. You are nothing more than livestock to them.”5 How Digital Identities Threaten Your FreedomDisguised as a tool for convenience and safety, digitized IDs, such as mobile driver’s licenses, “go way beyond what a driver’s license is about.”6 The World Economic Forum’s (WEF) Annual Meeting 2018 in Davos was focused on “advancing good, user-centric digital identities.”7 This isn’t simply a matter of maintaining your name, address and birthdate, or proof that you’ve passed your state’s driving exam. Digital identities are described by WEF as “complex webs, crossing the internet, of … personal data, digital history and the inferences that algorithms can draw from this.”8 These identities, they say, “are increasingly embedded in everything we do in our daily lives.” In a figure that describes digital identity systems in our everyday lives, WEF envisions that digital IDs, i.e., vaccine passports, will encompass:9
As an example of how this can translate to threatening something as foundational as your food choices, Lynn uses the example of the “entitlements digital currency” benefits program for food stamps in Illinois, which uses smart contracts and healthy eating tokens. She explains:10
22 Ways to Stop Vaccine PassportsYour entire identity, including your medical history, finances, sexual orientation and much more, could soon be stored in a mobile app that’s increasingly required to partake in society. While some might call this convenience, others would call it oppression. Many others are being driven by fear to accept vaccine passports as “necessary” to protect safety. In one survey that evaluated acceptance of vaccine passports, 60% stated they were in favor and only 20% stated they were strongly opposed. The study’s lead author, professor Stephan Lewandowsky, described those opposed as “surprisingly low,” adding, “It’s fascinating how people seem increasingly receptive to their personal data being used to inform themselves and others about what they can and can’t do.”11 There’s still time, however, to stop the imposition of totalitarian control worldwide, and a key way to do so is to fight back against vaccine passports. Lynn highlights 22 ways to do just, which we can all take part in to protect privacy, freedom and constitutional rights.12
from http://articles.mercola.com/sites/articles/archive/2022/01/26/ways-to-stop-vaccine-passports.aspx In mid-February 2021, Dr. Andrew Hill at Liverpool University published a scientific meta-analysis of six randomized controlled trials involving the use of ivermectin in 1,255 COVID-19 patients. (The paper was initially posted on a preprint server.) The review, which was funded by the World Health Organization and UNITAID, found that ivermectin increased viral clearance and reduced COVID-19 deaths by 75%. This is a rather massive benefit, yet the conclusion of the paper was dismissive, saying additional large clinical trials were needed to make a determination about whether or not to recommend its use. Hill Accused of Scientific MisconductIn early April 2021, Hill and his coauthors were accused of scientific misconduct by a French civic group called the Association BonSens. The TrialSite News video report from April 5 above reviews the details of this story. BonSens — labeled by some a “controversial group” based on its anti-mask mandate stance — accused Hill of data manipulation to downplay the usefulness of ivermectin. According to BonSens, Hill’s analysis was then used by the WHO to recommend against ivermectin, even though it appears to have significant benefit. BonSens called on Hill to retract the paper, but Hill remained “resolute and stands behind the study,” TrialSite News said. At the time, TrialSite News claimed to have been in conversation with “relevant and associated parties,” some of whom have asked to remain anonymous, who say Hill’s study was in fact modified, but that this was done “separate and apart from the investigator,” and that Hill had no say in the matter. However, since then, one of the six studies Hill included in his analysis has been withdrawn “due to fraudulent data.” In a public notice1 dated August 9, 2021, Hill and his coauthors addressed the matter, saying they would submit “a revised version excluding this study, and the currently posted paper will be retracted.” A revised and updated meta-analysis was published in November 2021.2 The updated review includes data from 23 randomized clinical trials with a total of 3,349 patients. Studies with “high risk of bias” were excluded. In this analysis, Hill found that “Ivermectin did not show a statistically significant effect on survival or hospitalizations,” and had only “borderline significant effect on duration of hospitalization in comparison with standard of care.” No significant effect on clinical recovery time was detected. In conclusion, the paper states that the WHO “recommends the use of ivermectin only inside clinical trials.” Curiously, it also states that “a network of large clinical trials is in progress to validate the results seen to date.” What results might those be? Surely, they must be referring to positive results, or else a network of clinical trials would hardly be justified. Positive Ivermectin Studies Largely Barred From PublicationDecember 3, 2021, TrialSite News interviewed Dr. Tess Laurie (above) about her own ivermectin analyses and that of Hill. She points out that she was concerned when she saw the initial meta-analysis Hill published, as the conclusion didn’t match the data. The reduction in death was significant, yet the conclusion was dismissive. Laurie contacted Hill, asking him to explain his conclusion to her. He then told her that the conclusion of the paper was not his own. It had been written by his sponsor — the WHO. Laurie was shocked, she said, as this struck her as a clear conflict of interest. In the interview, Laurie also discusses the general difficulty researchers have had, since the beginning, in getting papers published that support ivermectin. She admits her own team has downplayed the benefits by using extremely conservative analyses in an effort to get published.
Strong Evidence for IvermectinAccording to Laurie, the evidence for ivermectin in the treatment of COVID-19 is strong. In a previous interview, she reviewed a 13-study meta-analysis that found a 68% reduction in deaths. A follow-up review that included 15 studies found a 62% to 72% reduction in deaths.3 A meta-analysis4 by Laurie and her team published in the July-August 2021 issue of the American Journal of Therapeutics, which included 24 randomized controlled trials with a total of 3,406 participants, reported reductions in death ranging between 79% and 91%. A study published February 2021 also reported that a five-day course of ivermectin at a dose of 12 mg per day sped up viral clearance, reducing the duration of symptomatic illness by three days compared to placebo (9.7 days versus 12.7 days).5 According to Laurie, what makes ivermectin particularly useful in COVID-19 is that it works both in the initial viral phase of the illness, when antivirals are required, and in the later inflammatory stage, when the viral load drops off and anti-inflammatories become necessary. Dr. Surya Kant, a medical doctor in India who has written a white paper6 on ivermectin, claims the drug reduces replication of the SARS-CoV-2 virus by several thousand times.7 Kant’s paper led several Indian provinces to start using ivermectin, both as a prophylactic and as treatment for COVID-19 in the summer of 2020.8 Africa and Japan Defy the Odds With IvermectinJapan and Africa have also defied the odds with ivermectin. As reported by NewsRescue at the end of August 2021, “Melinda Gates, co-chair of the Bill and Melinda Gates foundation predicted disaster in the developing world, but so far she has been dead wrong, at least as far as Africa is concerned.”9 Indeed, despite having nearly 1.4 billion people, Africa has maintained one of the lowest COVID caseloads and death rates in the world, accounting for just 4% of the global reported death rate as of mid-May 2021.10 While media feign confusion, ivermectin may well be the explanation for this phenomenon. A study11 published at the end of December 2020 found that African countries that participated in the African Program for Onchocerciasis Control (APOC), where intensive ivermectin mass campaigns were carried out between 1995 and 2015, had 28% lower COVID-19 mortality and 8% lower infection rates than non-APOC countries that did not participate in the ivermectin campaign.
Similarly, Japan has seen a massive decline in cases after adopting ivermectin as standard treatment against COVID. November 3, 2021, Free West Media reported:13
Doctors Urge Acceptance of Ivermectin to Save LivesIn the U.S., the Frontline COVID-19 Critical Care Alliance (FLCCC) has been calling for widespread adoption of ivermectin, both as a prophylactic and for the treatment of all phases of COVID-19.14,15 FLCCC president Dr. Pierre Kory, former professor of medicine at St. Luke’s Aurora Medical Center in Milwaukee, Wisconsin, has testified to the benefits of ivermectin before a number of COVID-19 panels, including the Senate Committee on Homeland Security and Governmental Affairs in December 2020,16 and the National Institutes of Health COVID-19 Treatment Guidelines Panel January 6, 2021.17 As noted by the FLCCC:18
A one-page summary21 of the clinical trial evidence for Ivermectin can be downloaded from the FLCCC website. A more comprehensive, 31-page review22 of trials data has been published in the journal Frontiers of Pharmacology. At the time of this writing, the number of trials involving ivermectin has risen to 71, including 31 randomized controlled trials. A listing of all the ivermectin trials done to date, with links to the published studies, can be found on c19Ivermectin.com.23 The FLCCC’s COVID-19 protocol was initially dubbed MATH+ (an acronym based on the key components of the treatment), but after several tweaks and updates, the prophylaxis and early outpatient treatment protocol is now known as I-MASK+24 while the hospital treatment has been renamed I-MATH+,25 due to the addition of ivermectin. The two protocols26,27 are available for download on the FLCCC Alliance website in multiple languages. Take Control of Your Health CareIf COVID-19 were an actual medical crisis and not an excuse for a tyrannical power grab, doctors would have been allowed, indeed encouraged, to work together to find solutions. Their successes would then have been announced everywhere. Without doubt, ivermectin would have featured heavily in such reports, as doctors around the world have attested to its benefits. That’s not what happened, though, which tells us we’re not dealing with a medical crisis that governments actually want to solve. As reported by the FLCCC, its members have “been blocked in attempts to disseminate scientific information about ivermectin on Facebook and other social media with the FLCCC’s pages repeatedly being shut down.”28 Seasoned researchers like Laurie can’t get their research published, and the main thing they have in common is that they’re reporting positive results using ivermectin (and other common remedies). For nearly two years now, doctors and scientist have repeatedly shown we can control the COVID endemic, even with new variants. We can save the vast majority from severe illness and death. Yet “authorities” within government, regulatory agencies and health agencies have refused to listen and insist there’s only one way forward — we need novel gene transfer injections that direct our cells to churn out the very toxin that makes COVID-19 so problematic. And when those shots are proven failures, the answer, these same “leaders” say, is more boosters! Insanity is doing the same thing over and over, expecting different results. The good news is you can choose who you listen to. You can listen to frontline medical experts, like the FLCCC, and follow their advice. from http://articles.mercola.com/sites/articles/archive/2022/01/26/ivermectin-scientific-misconduct.aspx This article was previously published May 7, 2020, and has been updated with new information. Lying in the prone (face down) position, in which your chest is down and your back is up, could be a simple way to improve outcomes in cases of severe respiratory distress. This topic has received renewed attention during the COVID-19 pandemic, as invasive mechanical ventilation is conventionally delivered with the patient in the supine (face up) position, which refers to lying on your back. "Mechanical ventilation is the main supportive treatment for critically ill patients" infected with novel coronavirus 2019 (COVID-19), according to a February 2020 study published in The Lancet Respiratory Medicine.1 However, reports suggest that many COVID-19 patients put on ventilators don't make it. In a JAMA study that included 5,700 patients hospitalized with COVID-19 in the New York City area between March 1, 2020, and April 4, 2020, mortality rates for those who received mechanical ventilation ranged from 76.4% to 97.2%, depending on age.2 There are many reasons why those on ventilators have a high risk of mortality, including being more severely ill to begin with. However, given the poor outcomes, some physicians are now trying to keep patients off ventilators as much as possible by using alternative measures, including having patients lie on their stomachs (prone) to allow for better lung aeration.3 It's also possible that prone ventilation, which is ventilation delivered with the patient lying in the prone position, may help patients who aren't responding to conventional ventilation in the supine position,4 as well as reduce mortality in those with acute respiratory distress syndrome (ARDS).5 Prone Positioning Lowers Death Rate in Those With ARDSARDS is a lung condition that causes low blood oxygen and fluid buildup in the lungs. As fluid builds up in the lungs and surfactant, which helps the lungs fully expand, breaks down, the lungs are unable to properly fill with air.6 A person with ARDS will have shortness of breath, which can progress to low blood oxygen, rapid breathing and rattling sounds in the lungs when breathing. ARDS is a common complication among seriously ill COVID-19 patients, with one study suggesting that 100% of COVID-19 patients who died in one study were suffering from ARDS.7 In 2013, a study published in The New England Journal of Medicine found that early application of prone positioning may improve outcomes in people with severe ARDS.8 During the study, 466 patients with severe ARDS were randomly assigned to receive prone-positioning sessions of at least 16 hours or to stay in the supine position. After 28 days, 32.8% in the supine group had died, compared to 16% in the prone group. After 90 days, the supine group had a mortality rate of 41%, compared to 23.6% in the prone group, with researchers concluding, "In patients with severe ARDS, early application of prolonged prone-positioning sessions significantly decreased 28-day and 90-day mortality."9 Not only have previous studies found that oxygenation is significantly better among patients in the prone position compared to the supine position, but prone positioning may also prevent ventilator-induced lung injury.10 Why Prone Positioning Benefits ARDS PatientsIn the video above, Jonathan Downham, an advanced critical care practitioner in the U.K., explains why prone positioning can be so beneficial for those with ARDS. Using a simple example of a sponge filled with fluid, he shows how the direction of drainage changes depending on the sponge's position. In ARDS, the lung's air sacs, or alveoli, become damaged. Fluid leaks through the air sacs' damaged walls and collects.11 Fluid in the lung will increase its weight, which then squeezes out the gas from the dependent regions. If the sponge represents a fluid-filled lung, in the supine position the dependent regions are at the back of the lung. While the fluid in an ARDS patient's lung is more evenly distributed than the sponge model suggests, it helps to show how the increased lung mass squeezes out the gas of the gravity-dependent lung regions, and why the lung densities shift when moving from the supine to the prone position. According to Downham, this shift can occur in a matter of minutes after changing a person's position. Differences in shape of the lungs and chest wall also come into play. Lungs are normally conical, with the dependent side being the base and the non-dependent side being the apex. When supine, your lung is in this configuration. The chest wall, however, has a cylindrical shape, and because of this difference the lung must expand its upper regions more than the lower regions, which leads to a greater expansion of the nondependent alveoli and a lesser expansion of the dependent alveoli. Imagining that the lung is like a slinky, Downham then shows how, when a patient is in the prone position, the weight becomes much more evenly distributed, allowing for better ventilation. Taken together, when in the supine position, gravitational forces, increased pressure from the wet lung and shape-matching issues all combine to act in the same direction to have a detrimental effect on the dependent alveoli. The prone patient, however, suffers less from these effects. Other benefits also occur with prone positioning, including:
Prone positioning can also help with stress and strain on the lung, with stress referring to the tension in the fibrous skeleton when distending force is applied and strain being the volume increase caused by the applied force relative to the resting volume of the lungs. It also reduces lung inflammation in ARDS patients14 and may reduce the severity and the extent of lung injury caused by mechanical ventilation.15 Support for Early Use of Prone PositioningIncreasing research suggests that prone positioning should be used "systematically" in the early management of severe ARDS, and not reserved as a "rescue maneuver or a last-ditch effort."16 As noted by a pathophysiology-based review published in the World Journal of Critical Care Medicine:
The researchers suggested that prone positioning seemed to be beneficial in most cases of ARDS and recommended that "early use of prolonged prone positioning in conjunction with lung-protective strategies decreases mortality significantly."18 For best results, other researchers have suggested that prone ventilation sessions should last 12 to 18 hours per session and should be begun early, within 36 hours of diagnosis.19 A small study of patients with severe COVID-19-related ARDS who required mechanical ventilation in Wuhan, China, also revealed that lying in the prone position for 24-hour periods was better for the lungs.20,21 Unfortunately, despite the many potential benefits, prone positioning remains an underused technique. One study suggested that only 13.7% of patients with ARDS, and 32.9% of patients with severe ARDS, were placed in the prone position.22 Awake Proning Is Also BeneficialMuch of the research into prone positioning for respiratory distress has focused on its use during mechanical ventilation. However, at least one study has been planned to determine whether the use of prone positioning in awake self-ventilating patients with COVID-19-induced ARDS could improve gas exchange and reduce the need for invasive mechanical ventilation.23 Previous research also suggests that awake, spontaneously breathing patients who are not intubated can also benefit from prone positioning, which leads to improved oxygenation.24 Another study of care involving critically ill COVID-19 patients in China's Jiangsu Province recommended the use of awake prone positioning, which, the researchers noted, "showed significant effects in improving oxygenation and pulmonary heterogeneity."25 It's also been suggested that the physiological changes that occur with prone positioning may be even more favorable in spontaneously breathing patients than in those who are intubated. A 2003 study found, in fact, that the prone position led to a rapid increase in partial pressure of oxygen, or PaO2, which is a measure of how well oxygen moves from the lungs to the blood, among patients with respiratory failure.26 All of the patients in the study were able to avoid mechanical ventilation. In the case of COVID-19, some experts suggest that all patients who are awake and able to adjust their own position should use the prone position for two- to four-hour sessions, two to four times a day: How to Use Prone Positioning at HomeSome hospitals have also released instructions for self-proning, which can be used at home for people with cough or trouble breathing. If you're struggling to breathe, you should seek emergency medical care. However, in cases of cough or mild shortness of breath being treated at home, guidelines from Elmhurst Hospital recommend not spending a lot of time lying flat on your back.27,28 Instead, it suggests "laying [sic] on your stomach and in different positions will help your body to get air into all areas of your lung." The guidelines recommend changing your position every 30 minutes to two hours, including:
This is a simple way to potentially help ease breathing difficulties at home and, if you or a loved one is hospitalized, can be used there too. If your health care providers don't suggest it, ask whether prone positioning could help. from http://articles.mercola.com/sites/articles/archive/2022/01/26/prone-positioning-improves-survival-in-severe-ards.aspx At this point, there is simply no question. The COVID shots are an abysmal failure in every way possible. Again and again, data analyses from around the world show a negative correlation between “vaccination” rates and worsening infection rates and other health trends. There’s No Rationale for Passports and MandatesAmong the latest data sets to show this are official statistics from the U.K. government. Its “National Flu and COVID-19 Surveillance Report: 13 January 2022 (Week 2)”1 shows COVID infection rates in the U.K. are higher among the “fully vaccinated” in all adult cohorts. Infection growth rates are also rising faster among the fully vaxxed than in unvaccinated cohorts of all ages. All in all, these data prove that vaccine passports and mandates are completely pointless and nothing more than a coercion tool. In no way do they reduce infection rates, hospitalizations or deaths from COVID. Regardless of how many shots a person has received, they’re still getting infected and transmitting it. Plus, we know the jabbed are veritable incubators for mutating strains. Everything about this mass vaccination campaign is detrimental to public health. Far Higher Infection Rates Among the Fully JabbedUsing U.K. government data, a Twitter user named Don Wolt created a series of helpful graphs that he posted January 16, 2022.2 The graph below shows the differences in infection rates by age and vaccination status, and it is really telling. Across the board, with the exception perhaps of the 80+ age group, the fully jabbed have significantly higher rates of COVID infection, completely decimating the myth that we’re in a “pandemic of the unvaccinated.” Clearly, that is not the case. (Wolt clarifies that each bar in this graph represents four weeks of data, obtained from successive weekly U.K. HSA reports, and the chart illustrates the rates of infection — i.e., the number of infections per 100,000 people — not absolute numbers. “Vaxxed 2-doses” also includes those who have received a third booster.) 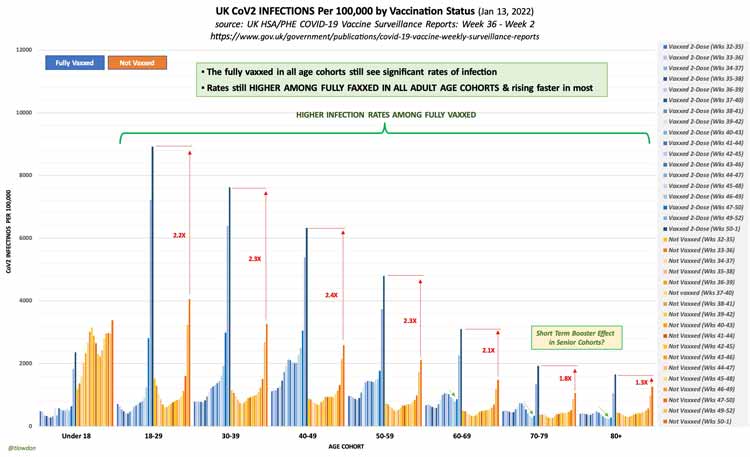 Infection Rates Rising Faster Among Fully JabbedIn another graph, you can clearly see how infection rates are also rising faster in fully jabbed cohorts than in the unvaccinated — and this is not a result of higher vaccination rates. Here, Wolt determined the growth of the infection rate for each age cohort by comparing the data of Week 1 against Week 2 in the surveillance report. As you can see by the orange graph bars, the growth rate of infection among the unvaccinated is relatively flat across age groups, whereas the infection growth rate among the fully jabbed keeps trending upward with age. As noted by Wolt, this infection growth rate increase is not due to a tandem increase in the number of people getting a second or third jab. The data show that the greater an age cohort’s vaccination rate is, the higher its infection growth rate (i.e., the rate of increase from one week to the next). 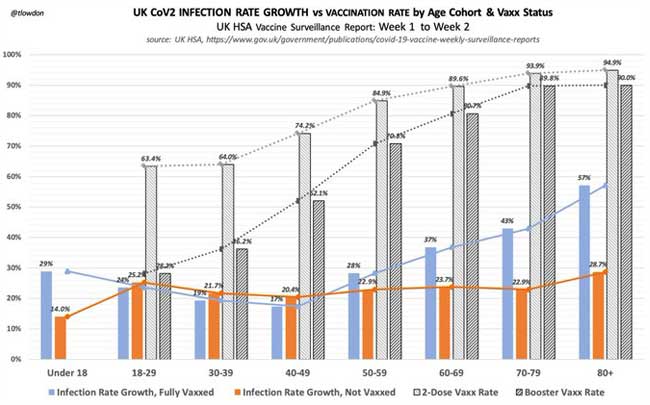 Risk of Death Is Extremely Low in Under-50 Age GroupsThe January 13, 2022, U.K. COVID surveillance report3 does show that, among those aged 50 and over, the COVID shots appear to lower hospitalization rates and death. However, anyone under the age of 50 who tests positive for SARS-CoV-2 infection still has an exceptionally low risk of hospitalization or death, regardless of vaccination status. In those under the age of 30, the risk of being hospitalized or dying from COVID is “effectively zero,” Wolt notes, which, again, “makes mandated vaccination utterly unwarranted.” 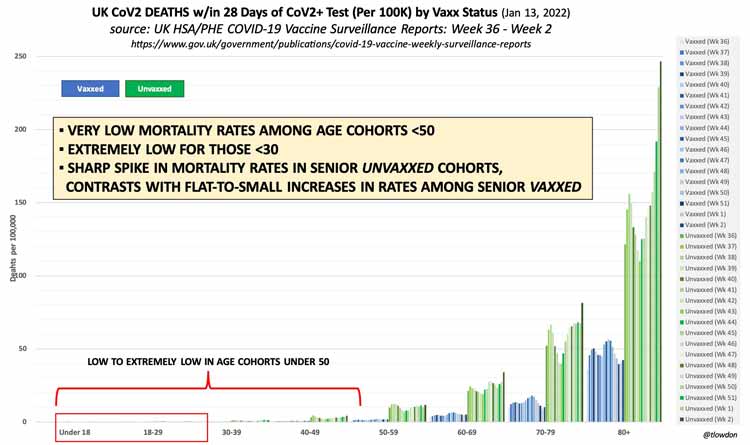 Responding to detractors who point out that the report warns its raw data cannot be used to estimate vaccine effectiveness, Wolt points out that his graphs are not meant to illustrate vaccine effectiveness per se. They merely show rate trends between “vaccinated” and unvaccinated, and these trends clearly invalidate any perceived need for vaccine mandates. Data from Scotland show more of the same. As reported by The Herald, January 13, 2022:4
Omicron Forces Media to Rethink What They ReportThe COVID pandemic has been all about social engineering, which of course cannot be done without the full complicity of the mainstream media. In a roundabout way, a January 12, 2022, AP News article5 admits this role:
Narrative Switch Aimed at Hiding FailuresFor those who have been “awake” to the censorship and misleading reporting over the past two years, this attempt at steering the narrative in a new direction is just laughable. How could the AP possibly have missed the fact that it’s been a data disaster from the start? And intentionally so? Case counts were always unreliable, considering the PCR test cannot diagnose an active infection, and excessive cycle thresholds guaranteed ridiculous amounts of false positives. COVID hospitalization data were always unreliable, because anyone who tested positive for COVID was counted as a COVID hospitalization whether they were symptomatic or not. Nothing has changed in that regard. The only thing that has changed is that now media are admitting it — pretending that this is a brand-new development, of course. The same goes for COVID death counts. They were vastly overcounted from the start, again, because of the reliance on faulty PCR testing. Media now claim to be moving away from “unreliable” data such as case counts, hospitalizations and even deaths, and for all the reasons we’ve been highlighting for the past two years. For those who have paid attention all along, this is clearly an attempt to change the narrative without losing all credibility (which I think is near-impossible at this point). The fact is that Omicron is making the holes in the narrative so much bigger, it’s all falling apart. They’re completely losing the rationale for vaccine passports and mandates for work, school and social events, as the higher the vaccination rate, the higher the infection rate. To that end, U.K. Prime Minister Boris Johnson announced January 19, 2022, that he was ending all remaining COVID restrictions in England,6 including mask mandates on public transportation and in schools, as well as vaccine passport requirements for public events. This is the complete opposite of what the technocrats need in order to justify passports and mandates. To hide, as best as possible, this narrative-killing trend, media are now “explaining” why they won’t be discussing case counts or even hospitalizations or death rates anymore. If they were, they’d have to admit that the pandemic response is resulting in an ever-growing disaster. So, don’t be surprised if fact checkers start debunking statistics proving what a disastrous failure the shots are by saying the data on cases, hospitalizations and deaths are simply too unreliable to use anymore. New Narrative Doesn’t Make Sense EitherThe new narrative, according to AP News, will highlight things like hospitals running over capacity and general staff shortages. The problem is, those don’t paint a true picture of COVID’s impact either, because hospitals have furloughed staff due to lack of patients (many have forgone routine medical treatments for fear of COVID), they’ve fired staff for not getting the jab, other staff have simply quit their jobs in the face of vaccine mandates and hospitals have shut down entire wings due to these staff cuts. Of course, if patients start returning, they might rapidly find themselves with more patients than they can currently handle. What else can you expect when hospitals intentionally make these kinds of cuts? General staff shortages in other industries are an equally flawed barometer of COVID’s impact. Many are still getting federal assistance and therefore don’t want to reenter the work force. Others are forced out due to vaccine mandates. Others are too sick to work thanks to COVID jab injuries. As recently reported by OneAmerica,7 a national mutual life insurance company based in Indianapolis, in addition to a 40% increase in deaths among working age Americans (and they’re not dying from COVID), there’s also been a noticeable uptick in short-term and long-term disability claims in the third quarter of 2021 compared to prepandemic levels. Working age Americans are getting too sick to work, and are dying at unprecedented levels, and it’s not because of COVID infection. ‘We Failed,’ Danish Media AdmitThe same attempt at switching the narrative can be seen in other countries. Danish media recently admitted they’ve failed the public by being “almost hypnotically preoccupied with the daily corona counts.”8 “We, the press, must ... take count of our own efforts,” Danish journalist Brian Weichardt writes, “And we’ve failed.” Weichardt admits that journalists failed to ask authorities for clear answers as to “what it meant in concrete terms that people are hospitalized with corona and not because of corona.” He also admits that this “makes a difference.” This, again, is precisely what many of us have been saying for the past two years, and all we got for the effort was a domestic terrorist label. Weichardt, in this piece, tries to shift the blame from journalists to the authorities themselves. They’re to blame, he thinks. “The messages of the authorities and politicians to the people of this historic crisis leave much to be desired,” he writes, ignoring the fact that a journalist’s No. 1 duty is to actually investigate, to double-check and to question, and not simply act as a two-legged parrot. For two years straight, any dissenting opinion has been labeled as dangerous misinformation, even when completely accurate, because that’s how propaganda works. The fact that press members are now starting to backtrack in order to save what little credibility they have left does not change the fact that they have, nearly universally, acted as promoters of propaganda and nothing else. Now that a majority of people are onto their spiel, they’re trying to pretend as though it were all a genuine mistake. Nice try. Let’s see how these pharma-backed propaganda jockeys fare when it comes to reporting the truth about COVID jab injuries. That will be where the rubber meets the road in terms of regaining credibility, as it will force them to bite the hand that feeds them — the drug industry. The sad truth is, we’re likely facing an avalanche of serious chronic ailments going forward, among them, neurodegenerative diseases, as detailed by Stephanie Seneff, Ph.D., in her article “SARS-CoV-2 Vaccines and Neurodegenerative Disease.”9 A short summation of this article reads as follows:
from http://articles.mercola.com/sites/articles/archive/2022/01/25/covid-vaccines-failure.aspx This article was previously published February 26, 2020, and has been updated with new information. Aside from causing a wide variety of side effects in those who take medications, the widespread routine use of pharmaceuticals also pose a serious risk to children who get their hands on them. As of 2016, nearly half the U.S. population was on at least one medication.1,2 Twenty-four percent used three or more drugs, and 12.6% were on more than five different medications.3 According to the 2016 National Ambulatory Medical Care Survey, 73.9% of all doctor's visits also involved drug therapy.4 As one would expect, drug use dramatically increases with age. As of 2016, 18% of children under 12 were on prescription medication, compared to 85% of adults over the age of 60. While this trend is troubling enough, with prescription drugs now being a staple in most homes, the number of children suffering accidental poisoning is also on the rise. Medications Pose Serious Risks to Young ChildrenIn September 2021 U.S. News and World Report announced that pediatric poisonings had risen dramatically during the pandemic.5 For example, Children’s Hospital of Philadelphia saw the number double just in the second half of 2020. The reason, health officials believe, is that with more people working from home, they have become more distracted or forgetful with their medicines than usual. Unfortunately, pediatric poisonings have been rising for several years. According to a 2012 article6,7 in The Journal of Pediatrics that reviewed patient records from the National Poison Data System of the American Association of Poison Control Centers, 453,559 children aged 5 or younger were admitted to a health care facility following exposure to a potentially toxic dose of a pharmaceutical drug between 2001 and 2008. In that time, drug poisonings rose 22%. Ninety-five percent of cases were due to self-exposure, meaning the children got into the medication and took it themselves, opposed to being given an excessive dose by error. Forty-three percent of all children admitted to the hospital after accidentally ingesting medication ended up in the intensive care unit, and prescription (opposed to over-the-counter) medications were responsible for 71% of serious injuries, with opioids, sedative-hypnotics and cardiovascular drugs topping the list of drugs causing serious harm. As noted by the authors:8
Keep All Drugs in Childproof ContainersIf you're older, you may recall your parents or grandparents would have a lockable medicine cabinet where drugs were stored. Few people keep their medications in locked cabinets or boxes these days, failing to realize the serious risk they pose to young children. The hazard is further magnified if you sort your medications into easy-open daily pill organizers rather than keeping each drug in its original childproof container. A 2020 paper9,10 in The Journal of Pediatrics, which sought to "identify types of containers from which young children accessed solid dose medications during unsupervised medication exposures" found 51.5% involved drugs accessed as a result of having been removed from its original childproof packaging. Remarkably, in 49.3% of cases involving attention deficit hyperactivity disorder medications and 42.6% of cases involving an opioid, the drug was not in any container at all when accessed. In other words, the child found the pill or pills just laying out in the open. In 30.7% of all cases where a child ingested a drug, the exposure involved a grandparent's medication. As noted by the authors:
Teen Drug Overdoses Are Also on the RiseWhile infants are notorious for putting anything and everything in their mouth, making them particularly vulnerable to accidental drug exposures, drug overdoses, particularly those involving opioids and benzodiazepines, are also becoming more prevalent among teens with access to these drugs. According to a 2019 study11 published in the journal Clinical Toxicology, 296,838 children under the age of 18 were exposed to benzodiazepines between January 2000 and December 2015. Over that time, benzodiazepine exposure in this age group increased by 54%. According to the authors:12
A similar trend has been found with opioids. A 2017 study13 looking at prescription opioid exposures among children and adolescents in the U.S. between 2000 and 2015 found:
Commonsense PrecautionsThe U.S. Centers for Disease Control and Prevention promotes and supports the Up and Away and Out of Sight campaign, which centers “around several simple, data-driven actions that parents and caregivers can take to prevent medication overdoses in the children they care about and care for.”14 These commonsense precautions include the following:15
What to Do in Case of Accidental Drug ExposureBe sure to keep the Poison Help number in your phone, and make sure your baby sitter or caregiver has it. In the U.S., the Poison Help number is 800-222-1222. If you suspect your child has taken a prescription or OTC medication, even if he or she is not yet exhibiting symptoms, call the Poison Help line immediately. If you're unsure what medication your child may have taken, call 911 or the emergency number in your area for transportation to the nearest medical facility. Although your child may appear fine in the initial minutes, this can rapidly change. You want to start treatment as soon as possible to reduce the risk of permanent damage or potential death. Remember to bring with you the names of any medications your child may have accidentally ingested, as well as any medications your child has taken in the past 24 hours as prescribed by their doctor, any allergies they have, and any changes or symptoms you may have observed. Unfortunately, symptoms of a medication overdose can vary widely, depending on the drug, dosage and age of the child. That said, symptoms of an overdose may include:16
Should your child exhibit any of the following symptoms, call 911 (in the U.S.) immediately:17
Opioid Epidemic Takes Toll on Pediatric PopulationIt’s crucial to realize that many drugs can be life threatening to a young child, even in low doses. This is particularly true for opioids and buprenorphine, a drug used to treat opioid dependence. As noted in a 2005 paper18 on opioid exposure in toddlers:
Similarly, a 2006 paper19 on the adverse effects of unintentional buprenorphine exposure in children noted that:
The take-home message here is that as drug treatment increases and becomes ever-more prevalent among all age groups, the risk of unintentional exposure increases as well. Toddlers will stick just about anything in their mouth, and young children will often not recognize there's a difference between pills and candy. As parents and caregivers, we simply must take the necessary precautions to keep all medications in a safe place, well out of reach of curious hands. Failure to safeguard your medications can have profoundly tragic consequences, so please, do not take this matter lightly. from http://articles.mercola.com/sites/articles/archive/2022/01/25/pediatric-medication-toxicity.aspx |
Nia Pure NatureThe Provider of premium Quality Health Products To Live Better Lives Archives
March 2022
Categories |
 RSS Feed
RSS Feed
