|
1 Which of the following may be a beneficial adjunct in COVID-19 treatment by reducing oxidative stress, counteracting hypercoagulation and breaking down blood clots? 2 What sets SARS-CoV-2 apart from other known coronaviruses? 3 Which of the following is currently the largest funder of the World Health Organization? 4 Which of the following has been shown to impact your risk of testing positive for SARS-CoV-2, illness severity, and COVID-19 mortality? 5 Which of the following doctors has developed two effective treatments involving vitamin C and steroids, one for the treatment of sepsis and another for COVID-19? 6 Genetic data suggests SARS-CoV-2 is a: 7 Which of the following can significantly increase your risk of serious COVID-19 infection? from http://articles.mercola.com/sites/articles/archive/2020/06/01/week-132-health-quiz.aspx
0 Comments
The unemployment caused by the coronavirus pandemic will soon exceed that of the Great Recession of 2007 to 2009 and represents the worst decline in jobs since the Great Depression in the 1930s.1 It is difficult to overstate how many jobs have been lost — each Labor Department report adds to the grim statistics. In two short months, the leisure and hospitality industry, which includes travel, tourism, lodging and recreation, shed almost half its jobs.2 Most of the lost jobs were related to eating and drinking establishments, work that depends on disposable income and the ability of people to move around freely.3 Bureau of Labor Statistics data, cited by Charles Gascon, regional economist for the Federal Reserve Bank of St. Louis suggest that more than 66.7 million people working in food preparation, sales, production and services are now at high risk of layoffs.4 Conventional food production and delivery have been severely disrupted, but what about natural foods? I am a founding member of an exciting plan to keep organic farmers and natural product businesses up and running during this difficult time. Are We Facing a Second Great Depression?During the Great Recession, the greatest economic downturn in recent times, unemployment peaked at 10% in October 2009.5 During the Great Depression of the 1930s, that figure was 24.9%, which included people in work relief jobs.6 When you compare those figures with estimates of unemployment rates that may come from the COVID-19 pandemic that are between 10.5% and 40.6%, you see how serious this is.7 Many of us did not live through the Great Depression, but we have seen pictures of the devastating poverty and heard stories from our older relatives. People lacked both food and money, and bread lines and soup kitchens were how many survived. According to U.S. History.com, the food offerings began as charity operations:8
Today, charities are still feeding the growing number of hungry people. A few weeks into the COVID-19 pandemic, U.S. food banks were swamped. At an Omaha food pantry that before the pandemic normally served 100 people a day, 900 people a day show up now.9 In Las Vegas, the Three Square Food Bank, which anticipated 200 to 250 cars a day through the pandemic, is getting up to a 4-mile-long caravan of 500 to 600 cars, according to The New York Times.10 Today's pandemic food shortages also have parallels to World War II. During the war, the cost of munitions and war-related items caused the producer price index to rise by 17% and consumer price index by 10%, which raised the price of everyday staples.11 This led to passage of the Emergency Price Control Act of 1942, which authorized the U.S. government to ration food and set prices.12 In addition to stabilizing prices, the Emergency Price Control Act was meant to prevent hoarding and price gouging and ensure that scarce resources could reach everyone evenly.13 Among the rationed items that Americans could buy only with coupon books were sugar, coffee, processed foods, meats, fats, canned fish, cheese and canned milk.14 Flash forward to today's pandemic and food is again being rationed, as well as paper products and hand sanitizers.15 Store shelves are sometimes bare and people wait in long lines outside of grocery stores. During World War II, there were few fast food restaurants and people usually ate at home. During this pandemic, while many fast food restaurants are seeing long lines, home cooked meals are again becoming the norm, creating more demand for dry good items like pasta. Big Food's Business Models Have Made Things WorseBig Food's large dairies, packing plants and concentrated animal feeding operations (CAFOs) are struggling during the pandemic as consumer demand wanes and their nonregenerative business models abysmally fail. Milk is being dumped and edible livestock euthanized even as people are struggling with hunger and food insecurity.16 It is a thorough indictment of conventional agriculture. According to Tim Gibbons, communications director at the Missouri Rural Crisis Center, COVID-19 is "shining a spotlight on the rigidity and lack of resilience for the corporate model of [farm production], which does not pay farmers fairly and is not good for consumers."17 It is ironic that despite the many systems' failures and even as Americans lose their livelihoods and face poverty, food insecurity and mental health crises, financial markets continue to rally. Ill-conceived government policies have clearly created a bubble that will crash in the future. Conventional, nonregenerative farming is responsible for virtually every major environmental and health problem we now have, including:
Job Losses Worsen Poor Countries' PlightsIn poor countries, COVID-19 presents even more dire consequences. People are not just at risk of illness and death with weak health care systems to treat them; they are also losing jobs because of the slowdown in Western countries' economies and less demand for the goods they manufacture and export. A half-billion people who were not living this way before the pandemic may be catapulted into poverty, says Oxfam, a conglomerate of 19 organizations working to end global poverty.18 That is a 6% to 8% rise in poverty for the entire global population. According to Oxfam:19
In Bangladesh, more than 1 million garment workers, most of whom are women, have been laid off without pay because of cancellations of orders from Western clothing brands.20 In Africa, it is estimated that as many as half of all jobs could disappear. A taxi driver and father told Oxfam he had not had passengers since the lockdown closed the airport and restaurants, and added "This virus will starve us before it makes us sick."21 In India, as many as half a million people who had been working outside their cities of origin literally walked back home after their jobs disappeared with the COVID-19 pandemic.22 Amitabh Behar, chief executive of Oxfam India, called the exodus the "largest mass migration since independence."23 In Delhi, throngs of displaced workers coalesce at food lines set up by the government to feed them, but the amount of food is not always sufficient. "Instead of coronavirus, the hunger will kill us," said Nihal Singh, a migrant worker hoping to be fed at one of the food lines,24 echoing the sentiments of the African taxi driver who spoke to Oxfam. Clearly, famine is following on the footsteps of COVID-19. The clustered food distribution in India and elsewhere also increases the risk of COVID-19 infections spreading, since the crowding and desperation of hungry people makes social distancing nearly impossible. Introducing ‘The Nourish Mint’ — A New Way ForwardEven though natural products have rarely been in greater demand from consumers, COVID-19 has prevented natural products’ industry conferences that were normally scheduled from occurring. Such meetings, like the Natural Products Expo West, usually held the first week of March, facilitate connections and allow raw ingredient companies to pitch to brands, and brands, in turn, to pitch to independent retailers. Until now. Luckily there is some good news when it comes to keeping the supply chain of natural foods and supplements flowing amid the temporary shutdown of such natural products’ industry conferences. The Organic & Natural Health Association has created a new way for farmers and natural product businesses to interface called "The Nourish Mint."25 The online events, the first to take place June 18 and 25, 2020, at 4 p.m. to 5 p.m. Eastern time, will allow:26
How does The Nourish Mint work? It will operate just like an in-person event in which raw ingredient companies and brands can present their products to an audience of independent retailers and other interested companies in the industry — except that it will be online. The presenters will have three minutes to showcase their products and three minutes to answer questions from the virtual audience.27 Flexibility is built into The Nourish Mint sessions. After the formal, live presentations of ingredients, products and brands, there will be an open social with attendees. Members of the audience will also be able to schedule individual or private meetings with the presenting companies for a future date. The Nourish Mint format is unique because it involves the entire supply chain, says Karen Howard, the CEO and executive director of Organic & Natural Health Association.28 How to Participate in a Nourish Mint EventCompanies that are interested in presenting at a Nourish Mint event can apply by sending pitch materials to [email protected], on or before June 2, 2020. For members of Organic & Natural Health Association, the cost to present to prospective buyers is $300 and for non-members, it’s $500. Only 20 companies will be chosen to present at the June 18 and 25 sessions.29 Among the industry expert audience, who are called "mintors," will be:30
Independent retailers who are members in good standing of SENPA, INFRA, Positively Natural and MAHO and Organic & Natural Health Association members may attend for free. Non-members may attend for $150 per session, and tickets can be acquired from the Organic & Natural Health Association.31 During the Pandemic Consider Growing Your Own FoodGrowing your own vegetables and fruits is one of the best ways to ensure ready access to fresh, nutrient-dense and chemical-free food. It especially makes sense during this pandemic with its economic and food disruptions. It is not true that you need a large space to grow a meaningful amount of food, though it is a popular misconception. In reality, "The Backyard Homestead" suggests you can grow enough organic food to feed a family of four on only a quarter-acre of land, all year round.32 In addition to supplying yourself with nutrient-dense, chemical-free food, a garden provides other important benefits. It gives you valuable and enjoyable physical exercise while exposing you to the UV rays so many people miss, especially during the COVID-19 shutdowns. Gardening is also a natural antidepressant and anxiety reducer. According to a meta-analysis in Preventive Medicine Reports:33
The COVID-19 pandemic has created unemployment, poverty, food insecurity and a likely economic depression. The Nourish Mint is a ray of hope and a new way forward for farmers and natural product businesses during these troubling times. from http://articles.mercola.com/sites/articles/archive/2020/06/01/the-nourish-mint.aspx As the number of people who have died from COVID-19 rises, more widespread testing reveals the infection may have moved farther and faster than was anticipated. The Centers for Disease Control and Prevention recently released five planning scenarios1 "designed to help inform decisions by modelers and public health officials who utilize mathematical modeling." Each of the scenarios is based on numerical values and epidemiological characteristics of the viral infection, reflective of data gathered before April 29, 2020. The CDC is clear these are estimates and not predictions:2
Although there was nearly immediate pushback,3 estimates from The Centre for Evidence-Based Medicine at the University of Oxford were similar.4 There were two numbers used to define the percentage of deaths. The case fatality rate was chosen to represent the number of deaths divided by the number of confirmed cases; it was limited by the number of people tested. Based on the possibility that up to 50% of those infected were asymptomatic, this created an abnormally high percentage. The infection fatality rate was used to represent the number of deaths divided by the number of people infected with SARS-CoV-2. That number was far lower since it included all people who are infected and not just those whose status was confirmed with a test. The Centre acknowledges that estimating fatality rates in the early stages of infection is subject to uncertainty. However, it's important to note that the infection fatality rate in the 3,711 passengers on the Diamond Princess cruise ship — the ship quarantined in Yokohama for 27 days at the start of the pandemic5 — was 1.3%.6 Quercetin Boosts Cellular Response to VirusesEven one death is too many. As I've written in the past, quercetin is a natural antihistamine and anti-inflammatory that lowers your risk for viral illnesses. In a recent paper, researchers identified one mechanism through which quercetin may work to control viral replication and promote health.7 Casein kinase II (CK2) is an enzyme with a diverse set of functions in the body. It is fundamental to controlling homeostasis at the cellular level. Yet, much of its functioning and mechanisms of action are still unknown.8 The enzyme is also involved in the survival and metastatic spread of cancer cells. There is evidence that it down-regulates the ability a cell has to generate type 1 interferon when attacked by a virus. It does this by inhibiting retinoic acid-inducible gene I (RIG-I),9 which has protein sensors that signal genetic expression of type 1 interferon by identifying the replication of RNA viruses, such as SARS-CoV-2. Researchers found that quercetin could inhibit the expression of CK2, which slowed the replication of RNA viruses in the lab and in mice.10 They pointed out that the effectiveness of supplemental quercetin may be hindered by the low solubility of the compound, which affects absorption. By using "enzymatically modified isoquercitrin (EMIQ)" they discovered they could develop plasma levels 20 times higher than the same intake of unmodified quercetin. The authors concluded quercetin or EMIQ "should be included" in aiding the control of viral infections. In research on the Ebola virus (EBOV) that triggered epidemics between 2013 and 2016, scientists found that the virus also suppressed type 1 interferon. They discovered that quercetin could suppress the effect on type 1 interferon and that it restored the body's ability to protect itself:11
What Are Interferons?Interferons (IFNs) are a subset of cytokines discovered in 1957.12 These cells are often the initial defense against viruses. There are two types and three forms of interferon. Within type 1 interferon, there are alpha and beta. Type II interferon has the gamma form.13 The different types are based on the function of the cytokine. Type I interferons help cells resist viruses. Type II aids in responding to infections and cancer growth. Initially, researchers hoped it could be used to treat diseases, including cancer. But it had serious side effects. After further development, several forms were released to treat genital warts, multiple sclerosis and hepatitis B and C with varying results. The name "interferon" came from the ability of Type 1 to interfere with the virus's ability to duplicate. A cell secretes interferons when a foreign substance, like a virus, is detected. However, the interferon does not function by attacking the virus. Instead, it tells the infected cell and the cells that surround the infected cell to make proteins that stop viral replication. Quercetin functions to stop CK2 from interfering with the action of type 1 interferon so cells are signaled to stop viral replication. Quercetin Works With Zinc to Stem Viral ReplicationQuercetin also functions as a zinc ionophore. This is a substance that helps transport zinc through the cellular plasma membrane14 and raises the level of zinc inside the cells. It's another mechanism through which quercetin may help lower the viral load and reduce the severity of viral infections. Zinc has proven antiviral properties and can reduce the length of the average cold by 33%.15 Recently, scientists pointed out there were indications that maintaining normal zinc levels may help reduce the severity of COVID-19.16 In the lab, zinc has demonstrated the ability to inhibit replication of the SARS-CoV-2 virus, which researchers believe is the underlying therapeutic effect in the use of hydroxychloroquine. Zinc may also up-regulate interferon production and the antiviral activity of the protein. Experts think it may reduce the risk of a secondary bacterial infection, especially against Streptococcus pneumoniae. Interestingly, zinc deficiency is common in older adults and in those who are obese, have diabetes or atherosclerosis. Likely not by coincidence, these are some of the same populations who have a higher risk of severe disease from SARS-CoV-2.17 The research team who looked at past studies on zinc suggest that it has a protective effect against COVID-19 by lowering inflammation, helping clear mucus, preventing ventilator-induced damage and supporting immunity.18 In addition to the impact quercetin has on the immune system, researchers have also found it helps to ameliorate obesity, Type 2 diabetes, circulatory dysfunction, chronic inflammation and seasonal allergies.19 It has also been found to help lower blood pressure in patients with Stage 1 high blood pressure.20 Researchers have found that quercetin can trigger tumor regression and it can activate the mitochondrial pathway of apoptosis.21 This is programmed cell death, without which cells can grow uninterrupted and develop into cancerous growths. Hydroxychloroquine: Poor Outcome With Added RiskTwo recent trials with the antimalarial drug hydroxychloroquine have yielded disappointing results. The first 75 patients at 16 Chinese treatment centers who were positive for COVID-19 were given hydroxychloroquine.22 The researchers found the primary endpoint of a reduction in the viral load, and secondary endpoints of improvement and reduction in clinical symptoms, were not significantly better than in the control group. The group receiving hydroxychloroquine had a negative conversion of 85.4% compared to the control group of 81.3%. In addition, the group receiving hydroxychloroquine had a greater number of adverse events compared to the control group. The most common was diarrhea. The authors concluded:23
In a second study published in the Lancet,24 researchers used a multinational registry of patients who were given hydroxychloroquine or chloroquine, with or without a macrolide antibiotic for treatment. This class of antibiotic includes azithromycin, which has been used in other study groups. There were 671 hospitals over six continents that supplied data of patients who were hospitalized between December 20, 2019, and April 14, 2020. During the study period there were 96,032 patients who met the criteria; 14,888 were in the treatment group and 81,144 were in the control group. After controlling for confounding factors, the mortality rates were compared, and the researchers were unable to find a benefit from the antimalarial drugs when they were used alone or with a macrolide. What they did find was that using the:25
A third observational study, published in The New England Journal of Medicine, found using hydroxychloroquine did not improve patient outcomes with COVID-19.26 In addition the FDA has cautioned against the use of hydroxychloroquine or chloroquine as an outpatient related to the dangerous heart arrhythmia side effects from the drugs.27 What is important to note in each of these studies is the absence of zinc in the intervention groups. We now know that chloroquine and hydroxychloroquine are zinc ionophores,28 which means the main ingredient required to prevent the viral infection may not have been given. While it is difficult to make an assumption of the efficacy of treatment of COVID-19 with hydroxychloroquine, since zinc was not given in each of these studies, it is also important to consider the secondary side effects associated with the drug, namely ventricular arrhythmias. Dose Recommendations for Zinc and QuercetinDuring the COVID-19 pandemic and future infectious disease seasons, supplementing with quercetin and zinc may be a good idea for many. It can help boost your immune system's innate ability to ward off infectious illness. As for dosage, here are some basic recommendations: • Quercetin -- According to research from Appalachian State University in North Carolina, taking 500 mg to 1,000 mg of quercetin per day for 12 weeks results in "large but highly variable increases in plasma quercetin … unrelated to demographic or lifestyle factors."29 • Zinc (and copper) -- When it comes to zinc, remember more is not better. In fact, it can backfire. When taking zinc, you also need to be mindful of maintaining a healthy zinc-to-copper ratio. Chris Masterjohn has a Ph.D. in nutritional sciences.30 He's written about the relationship between zinc and copper, saying:31
from http://articles.mercola.com/sites/articles/archive/2020/06/01/quercetin-lowers-your-viral-infections-risk.aspx As reviewed in “Vitamin D Level Is Directly Correlated to COVID-19 Outcomes,” there’s compelling evidence to suggest optimizing your vitamin D level can reduce your risk of COVID-19 and other viral infections such as seasonal influenza. A number of different scientists are calling for people and governments to prepare for a second wave of COVID-19 come fall, both in the U.S. and abroad.1 Considering SARS-CoV-2 has been shown to be responsive to temperature and humidity, with infectiousness increasing with lower temperatures and humidity levels, we’re likely going to see a reemergence of COVID-19 infections in the fall, during normal influenza season. REALLY IMPORTANT: Optimize Your Vitamin D Level Before Fall!What this means is you now have a known “deadline” for optimizing your vitamin D level. To improve your immune function and lower your risk of viral infections, you’ll want to raise your vitamin D to a level between 60 nanograms per milliliter (ng/mL) and 80 ng/mL by fall. In Europe, the measurements you’re looking for are 150 nanomoles per liter (nmol/L) and 200 nmol/L. Historically, December typically has highest flu activity in the U.S.,2 but it would probably be good to aim for October, or maybe even earlier depending on your location. Optimizing your vitamin D is particularly important if you have darker skin, as darker skin places you at higher risk for vitamin D deficiency — and serious COVID-19 infection. COVID-19 Racial Disparity Rooted in Vitamin D DeficiencyAs reported by The Guardian,3 the COVID-19 mortality among black Americans is three times higher than that of whites, and researchers have long known that blacks cannot achieve optimal vitamin D levels from sun exposure at any time of the year in Northern America.4 Research5 posted April 28, 2020, points out that vitamin D insufficiency is prevalent in severe COVID-19 cases and that “Emerging health disparities data regarding African-American and homeless populations suggest that vitamin D insufficiency (VDI) may be an underlying driver of COVID-19 severity.” Importantly, this study6 found 100% of COVID-19 patients under the age of 75 admitted to intensive care units had vitamin D insufficiency. A letter to the editor,7 published in the Irish Medical Journal, also points out the many links between vitamin D deficiency and factors known to play a role in COVID-19, such as male sex, acute respiratory distress syndrome (ARDS) and comorbidities like obesity, diabetes and heart disease, and presents data from an in-hospital review of 33 male COVID-19 patients’ vitamin D levels. The 12 patients who progressed to ARDS had a mean vitamin D level of 27 nmol/L (10.8 ng/mL), whereas those who did not progress to ARDS had a mean level of 41 nmol/L (16.4 ng/mL). It’s worth noting that 16.4 ng/mL is still grossly insufficient, as 40 ng/mL (100 nmol/L) has been established as a minimum level of sufficiency for general health and disease prevention by GrassrootsHealth.8 The same goes for the elderly, as you tend to lose the ability to convert vitamin D from sun exposure as you age. Step 1: Measure Your Vitamin DSo, how do you go about optimizing your vitamin D level? First, you need to find out what your base level is, which is done using a simple blood test. An easy and cost-effective way of doing this is to order GrassrootsHealth’s vitamin D testing kit. Once you know what your blood level is, you can assess the dose needed to maintain or improve your level. Again, the ideal level you’re looking for is above 40 ng/mL, and ideally between 60 ng/mL and 80 ng/mL (European measurement: 100 nmol/L or, ideally, 150 nmol/L to 200 nmol/L). The easiest way to raise your level is by getting regular, safe sun exposure, but if you’re very dark-skinned, you may need to spend about 1.5 hours a day in the sun to have any noticeable effect. Those with very light skin may only need 15 minutes a day, which is far easier to achieve. Still, they too will typically struggle to maintain ideal levels during the winter. So, depending on your situation, you may need to use an oral vitamin D3 supplement. The next question then becomes, how much do you need? Step 2: Assess Your Individualized Vitamin D3 DosageThe reason you do not want to get fixated on arbitrary dosage recommendations is because the required dose can vary greatly depending on several factors, including skin color, weight and other nutritional deficiencies. As explained by GrassrootsHealth:9

While this chart provides a starting point, you can fine-tune your dosage further by taking into account your baseline vitamin D level. To do that, you can either use the chart below, or use GrassrootsHealth’s Vitamin D*calculator. To convert ng/mL into the European measurement (nmol/L), simply multiply the ng/mL measurement by 2.5. 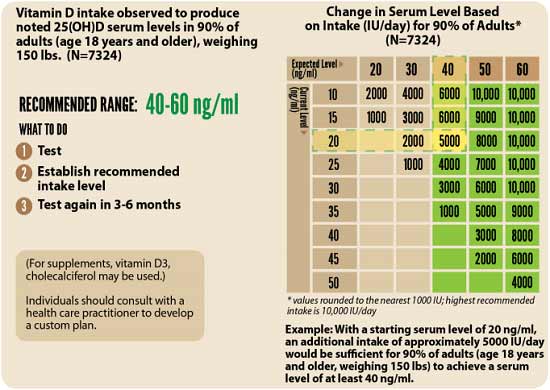
How to Calculate Your Vitamin D From Sun ExposureTo calculate how much vitamin D you may be getting from regular sun exposure in addition to your supplemental intake, consider using the DMinder app,10 created by Dr. Michael Holick, author of “The Vitamin D Solution: A Three-Step Strategy to Cure Our Most Common Health Problems.” The free app is available for iPhone and android in the Apple store and Google play respectively. As explained by imedicalapps.com:11
Step 3: RetestNext, you’ll need to re-measure your vitamin D level in three to six months, to evaluate how your sun exposure and/or supplement dose is working for you. As explained by GrassrootsHealth:
What Is the D*action Project?Aside from the DMinder app, another helpful tool is the myData-myAnswers online tracker created by GrassrootsHealth. You automatically have access to this tool when you buy their vitamin D testing kit and enroll in the D*action project. You can track any given supplement with this tracker (not just vitamin D). By tracking exactly how much you take and when, you can get a clearer picture of your personal requirement to reach and maintain an ideal level. When you buy the GrassrootsHealth testing kit, you agree to enroll in the D*action project, an international field study aimed at solving the vitamin D deficiency epidemic. By sharing your test results and anonymized personal health data with GrassrootsHealth researchers, you will enable them to determine the details of how vitamin D impacts health. As explained by GrassrootsHealth:
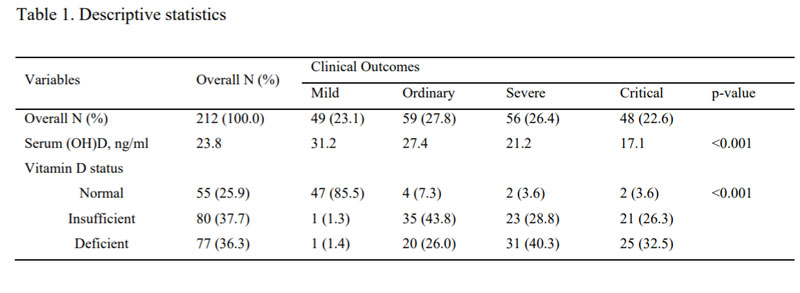
While I make these testing kits available in my online store, I do not make any profit from their sale. All proceeds go directly to GrassrootsHealth. If you prefer, you can also obtain the kit directly from their website. Share and Inform Your CommunityI urge everyone to share this information with friends, family and community at large, so that we can minimize a second outbreak. For example, you could speak to pastors in churches with large congregations of people of color and help them start a program getting people on vitamin D. Doing so could help save many lives; far more than any vaccine program. Additionally, if you have a family member or know anyone that is an assisted living facility, you could meet with the director of the program and encourage them to get everyone tested or at least start them on vitamin D. from http://articles.mercola.com/sites/articles/archive/2020/06/01/vitamin-d-level-to-reach-before-covid-19-second-wave.aspx In this interview, I interview three vitamin D experts about the importance of vitamin D for improving your immune function and resistance to viral infections of all kinds, including COVID-19. Bruce Hollis, Ph.D., with the Medical University of South Carolina, has researched vitamin D since the late 1970s. His research associate at the Medical University of South Carolina is Dr. Carol Wagner, who is a neonatologist and has been researching vitamin D since 2000. Carole Baggerly is the director and founder of GrassrootsHealth Nutrient Research Institute, a nonprofit public health research organization dedicated to moving public health messages regarding vitamin D from research into practice. Baggerly received our Game Changer Award in 2018. She started her work in vitamin D after treatment for breast cancer in 2005. Vitamin D Levels Correlate With Disease SeverityGrassrootsHealth recently conducted a review of an observational study involving 212 patients in Southeast Asia who had COVID-19, identifying a correlation between vitamin D levels and disease severity. Those with the mildest disease had the highest vitamin D levels, and vice versa. Of the 212 people, 49 had mild disease; 59 had ordinary disease; 56 were severe and 48 were critical. In the initial study group of 212 patients (see Table 1 below), 55 had normal vitamin D levels, which was defined as greater than 30 ng/ml; 80 had insufficient levels of 21 to 29 ng/ml and 77 had deficient levels of less than 20 ng/ml. Now, it’s worth noting that the “optimal” vitamin D level in that study was set at 30 nanograms per milliliter (30 ng/mL), which may actually be suboptimal. According to the research done by GrassrootsHealth, 40 ng/mL is the lower edge of optimal, with 60 ng/mL to 80 ng/mL being ideal for health and disease prevention. Despite that, the benefit of having a vitamin D level above 30 ng/mL was clear. 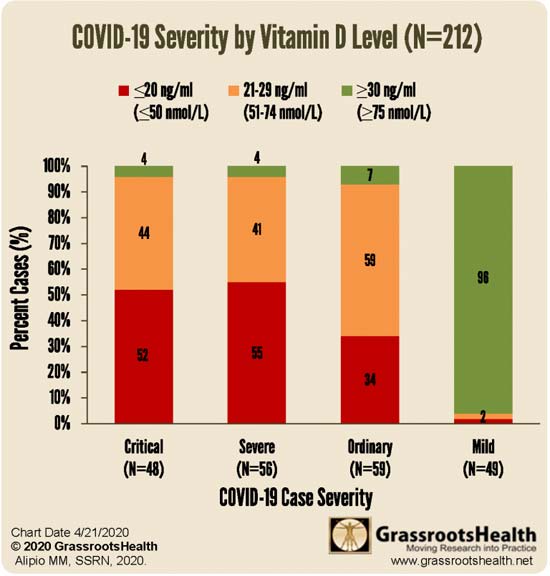
Vitamin D Levels Correlate With Mortality RiskA second study looked at the data from 780 hospital patients in Indonesia. The same vitamin D level cutoffs were used in this study: below 20 ng/mL; between 20 ng/mL and 30 ng/mL; and above 30 ng/mL. After adjusting for confounding factors, those with a vitamin D level between 20 ng/mL and 30 ng/mL had a sevenfold higher risk of death than those with a level above 30 ng/mL. Having a level below 20 ng/mL was associated with a 12 times higher risk of death. As noted by Hollis, “That's really strong data.” It’s Your Vitamin D Blood Level That Matters, Not the DoseNow, many vitamin D studies conclude that vitamin D supplementation has little or no effect on any given health problem or condition. But there’s a very simple reason for this: Virtually every one of these studies use the same dosage or dosages for everyone, and do not measure participants’ blood levels. This is a crucial mistake, as it’s really the blood level that needs to get over a particular threshold, and the dosage required to get there can vary widely. Another problem is the fact that most studies use far too low a dosage. If the dosage is too low, you cannot get your blood level into the protective range, and thus it will appear as though vitamin D is useless. A third factor that can influence the outcome of vitamin D studies is the interaction between vitamin D and other nutrients. Competing deficiencies can affect a particular sub cohort or population, thereby obfuscating results. A fourth factor is how you define deficiency — using a “word” versus a serum level. For the GrassrootsHealth Scientists’ Panel of 48 researchers, the consensus is that minimum serum level should be 40 ng/ml (100 nmol/L). Wagner explains:
Hollis adds:
Laws Need UpdatingUnfortunately, with labeling laws the way they are, it’s very difficult to get this point across. As noted by Baggerly:
Skin Color Impacts Your Vitamin D Deficiency RiskThe color of your skin has correlations to your vitamin D level, and we’re also seeing racial disparities in COVID-19. As noted by Hollis, in Detroit, Michigan, where African-Americans account for 14% of the population, they accounted for 40% of COVID-19 deaths.1
Vitamin D deficiency likely plays a role in this racial disparity, although nutrition, obesity and diabetes rates also contribute to immune dysfunction. It’s important for people with darker skin to realize that the more melanin you have, the more sun exposure you require to make sufficient amounts of vitamin D. According to Hollis, it’s physiologically impossible for a dark-skinned individual in the United States, unless they're in Southern Florida or Hawaii, to get optimal vitamin D from typical sun exposure. Daily Supplementation May Strengthen Lung TissueIf for whatever reason you cannot get regular sun exposure, then vitamin D supplementation is advisable. Ideally, you’ll want to take it daily, opposed to taking a large bolus dose once a week or once a month. As noted by Hollis, studies have consistently shown only daily supplementation were effective.
Baggerly adds:
Vitamin D3’s ability to strengthen the endothelial structure of the lungs may be one way in which vitamin D helps protect against COVID-19. “COVID-19 attacks the lungs … and vitamin D in this model showed to stabilize that,” Hollis says. Vitamin D Strengthens and Regulates Immune FunctionVitamin D also has a clear effect on your innate immune system, which is your first line of defense against bacteria and viruses, as well as your adaptive immune system, which involves your T regulatory helper and suppressor cells, and natural killer cells. All of these need to be in balance, Wagner explains. If an imbalance occurs, you can end up with a cytokine storm. According to Wagner, vitamin D is very effective for regulating and balancing adaptive immunity. One example demonstrating the elegance of this system is pregnancy. Wagner explains:
Research has also demonstrated that pregnant women with optimal vitamin D levels significantly reduce their child’s risk of developing Type 1 diabetes, which is an autoimmune disorder. As noted by Baggerly:
The Importance of Vitamin D TestingNaturally, vitamin D has many other benefits beside boosting immune function and protecting against respiratory diseases and viral infections. Wagner, for example, reviews some of the benefits in pregnancy and delivery, so for more information, be sure to listen to the interview. As mentioned, the most important factor here is the level of vitamin D in your blood, not the daily dose, so it’s important to get tested at least twice a year. Again, you want a level of at least 40 ng/mL, and ideally between 60 ng/mL and 80 ng/mL. According to data published in the Archives of Internal Medicine,2 75% of American adults and teens are deficient in vitamin D, based on a sufficiency level of 30 ng/mL. If the sufficiency cutoff were to be moved to 40 ng/mL or 60 ng/mL, deficiency rates in the U.S. would likely be in the high 90% bracket. Importantly, aside from people with darker skin, the elderly tend to lose the ability to synthesize vitamin D from sun exposure, and therefore tend to have suboptimal levels even if they spend plenty of time outdoors. “It's at that point people may need to supplement or find additional sources,” Baggerly says. One of the easiest and most cost-effective ways of measuring your vitamin D level is to participate in the GrassrootsHealth’s personalized nutrition project, which includes a vitamin D testing kit, either alone or in combination with the omega-3 test. This is done in the convenience of your home. You’ll learn your nutrient levels, how effective your health actions are, and you’ll be able to see 1000’s of other data sets that allow you to compare health outcomes important to you. The Synergy Between Magnesium and Vitamin DIf your vitamin D level is low and remains low even though you’re taking high dosages every day, say around 5,000 to 10,000 IUs, you may be too deficient in magnesium for your body to convert the vitamin D into its active form. As explained by Hollis:
GrassrootsHealth now also has a magnesium research project called Magnesium* PLUS Focus, which is also open for enrollment. All of these nutrient field trial projects involve sending in a blood spot test that you do at home, and filling out a health questionnaire and providing details on the supplements you take. COVID-19 Study UnderwayLast but not least, GrassrootsHealth is currently working on a vitamin D study to assess its ability to prevent COVID-19 and/or reduce illness severity. Wagner explains:
REALLY IMPORTANT: Optimize Your Vitamin D Levels Before Fall!Not only will be this an important strategy for you and your family, but it would be really helpful to start thinking about your community. People of color are at really high risk because their skin color impairs their ability to generate vitamin D from sun exposure. So if you could speak to any pastors in churches with large congregations of people of color and help them start a program getting people on vitamin D you could help save many lives, far more than any vaccine program. Additionally, if you have a family member or know anyone who is in an assisted living facility you could meet with the director of the program and encourage them to get everyone tested or at least start them on vitamin D. Tomorrow I will have an article with more specific action steps, so you can start planning now. For years, I’ve stressed the importance of optimizing your vitamin D level, especially in anticipation of flu season, and it seems clear it can go a long way toward protecting yourself against COVID-19 as well. Wagner notes:
In closing, experts are already warning that SARS-CoV-2 may reemerge in the fall when temperatures and humidity levels drop, thereby increasing the virus’ transmissibility. Now is the time to check your vitamin D level and start taking action to raise it if you’re below 60 ng/mL. Again, an easy and cost-effective way of measuring your vitamin D level is to order GrassrootsHealth’s vitamin D testing kit and learn more about vitamin D and its impact on your health. Knowledge is empowerment, and that is particularly true during this pandemic. from http://articles.mercola.com/sites/articles/archive/2020/05/31/vitamin-d-combats-viral-infections-boosts-immune-system.aspx As reported in "Bioweapon Labs Must Be Shut Down and Scientists Prosecuted," there's mounting evidence suggesting SARS-CoV-2 may have been leaked (whether inadvertently or not) from the biosafety level (BSL) 4 laboratory in Wuhan, China. Secretary of State (and former CIA chief) Mike Pompeo has gone on record stating "the coronavirus originated in a lab in Wuhan," and has accused China of covering up the leak.1,2 I've also interviewed bioweapons expert Francis Boyle and molecular biologist Judy Mikovits, both of whom have cited evidence that strongly points toward SARS-CoV-2 being an escaped laboratory creation. Why Was Wuhan Lab Shut Down?Fueling suspicions that SARS-CoV-2 escaped from the lab in Wuhan — and that it began far earlier than admitted — is an analysis3 of commercial telemetry (i.e., cellphone) data showing a significant and unusual reduction in device activity in and around the Wuhan Institute of Virology's (WIV) National Biosafety Laboratory during October 2019.4,5,6 According to the open source telemetry report,7 "Beginning on October 11, there was a substantial decrease in activity," and "the last time a device is active prior to October 11 is October 6." Between October 14 and October 19, there was no device activity in the area around the laboratory at all. "During this time, it is believed that roadblocks were put in place to prevent traffic from coming near the facility," the report states. What's more, between October 7 and October 24, there was no activity within the facility itself. While not concrete proof of a biohazard leak, the absence of cellphone traffic in and around the laboratory in October 2019 suggests the lab may have been shut down for a period, and the roads around it blocked off. The question is why? Amid accusations that the World Health Organization helped suppress information about the pandemic on behalf of China, a review of its handling of the COVID-19 pandemic will be conducted,8 although it is still unclear which body will conduct the review and when. Many are also asking just how independent such a review will or can be. What Kinds of Experiments Were Done at Wuhan Lab?A crucial piece of the lab release hypothesis that is missing from media reports and scientific opinion is a clear description of the experiments being conducted at the WIV. WIV researchers have engineered chimeric viruses where the gene for the cell entry protein (S protein receptor-binding domain) from one virus is replaced by that of another virus. In a May 16, 2020, article,9 Fabio Carisio, founder and editor-in-chief of the Italian Christian news site, GospaNews, reviewed, in chronological order, experiments involving chimeric superviruses conducted at WIV and the governments that funded them. As described in one 2017 study published in PLOS Pathogens,10 "Cell entry studies demonstrated that three newly identified SARSr-CoVs with different S protein sequences are all able to use human ACE2 as the receptor, further exhibiting the close relationship between strains in this cave and SARS-CoV." The goal of these experiments has been to identify what determines a virus' ability to enter into a human cell. The extension of these experiments is to infect living animals with these chimeric viruses to evaluate the factors that determine disease symptoms and spread. One of the authors of that 2017 PLOS Pathogens study was Dr. Shi Zheng-Li, director of WIV, also known as the "bat woman," as she's been China's leading researcher of bat coronaviruses.11 Zheng-Li and WIV have had a long-standing collaboration with Peter Daszak, Ph.D., and the EcoHealth Alliance Inc. in New York City, which Daszak is also the president of.12 EcoHealth Alliance is a U.S. pandemic prevention group. Daszak is also chairman of the Forum on Microbial Threats at the National Academies of Sciences, Engineering and Medicine,13 a private nonprofit that advises government on scientific matters and is funded by Congress, federal agencies and philanthropic organizations.14 Daszak is currently leading a project to continue these potentially dangerous animal experiments,15 and it's worth noting that he has also been one of the most prominent and vocal critics of the lab release hypothesis. On a side note, 60 Minutes recently reported16 the White House Administration cut Daszak's funding in late April 2020 — funding that, according to Daszak, had been instrumental during Gilead's development of the antiviral drug Remdesivir,17 which is now being promoted as a treatment for COVID-19. Remdesivir's development was sponsored by the National Institute of Allergy and Infectious Diseases (NIAID), which is led by Dr. Anthony Fauci. Fauci is also a board member18 of the Global Preparedness Monitoring Board (GPMB). GPMB is an organization that claims to be an independent monitoring and accountability body but is in fact part and parcel of the World Health Organization and The World Bank, and receives funding from the Bill & Melinda Gates Foundation.19 You can learn more about these sordid connections, and why they matter, in "Global Health Mafia Protection Racket." Another Paper Questions Natural Evolution TheoryAs mentioned, a number of experts have weighed in on the science of SARS-CoV-2's origin by analyzing its genetic code. Perhaps two of the clearest expositions on this have been published by Chris Martenson,20 Ph.D., and Yuri Deigin.21 Another paper prepublished May 2, 2020, ahead of peer-review, points out:22
Anonymous Scientist Accuses Zheng-Li of Scientific FraudGetting back to Zheng-Li, she increasingly appears to be a key figure in the discussion as to whether SARS-CoV-2 is of natural origin or not. January 23, 2020, she published a paper23 in the journal Nature, titled "A Pneumonia Outbreak Associated with a New Coronavirus of Probable Bat Origin," in which she compared the genetic sequence of SARS-CoV-2 to other coronaviruses and delineated its evolutionary path. According to Zheng-Li and her co-authors, SARS-CoV-2 "is 96% identical at the whole-genome level to a bat coronavirus" called RaTG13. They further claim they could find "no evidence for recombination events was detected in the genome of 2019-nCoV."24 The disturbing thing about this bat coronavirus, RaTG13, is that it appears to have the ability to infect humans. These findings are now being rebuked by an anonymous — possibly Chinese — researcher who has published25 an alternative theory in a blog called Nerd Has Power and refers to him or herself as "A nobody scientist."26 The blog post in question has been discussed by GM Watch,27 Australian science writer Joanne Nova28 and Steven Mosher,29 president of the Population Research Institute (a nonprofit research group that exposes human rights abuses and the myth of overpopulation30), who noted that:
The unnamed blogger writes, in part:31
Was Evidence for Natural Evolution Fabricated?In other words, this anonymous individual claims Zheng-Li fabricated the genetic code of the RaTG13 virus, and that it doesn't actually exist. The blogger points out that had Zheng-Li in fact discovered a bat coronavirus in 2013 capable of infecting humans, it would have been a groundbreaking discovery. Alas, she never published such a paper. Instead, she "made her fame in the coronavirus field by publishing in Nature32 two bat coronaviruses (Rs3367 and SHC014)," the unnamed blogger writes.33 That paper, published in 2013, showed SARS was likely of bat origin, and that it uses the ACE2 receptor for cell entry.
The blogger then goes on to dissect the genetic sequence RaTG13's spike protein, which "reveals clear evidence of human manipulation." (Again, Mosher offers a layman's overview35 of the data.) Martenson36 and Deigin's37 reviews of the viral genome also focus on the S2 spike protein, but they both focus on the spike protein found in SARS-CoV-2 (not the RaTG13 spike). According to Martenson, the fact that SARS-CoV-2's spike protein has a furin cleavage site is "the smoking gun" that proves it was created in a lab. I invite you to review his easy-to-follow analysis in "The Smoking Gun Proving SARS-CoV-2 Is an Engineered Virus." If the Nerd Has Power blogger is correct, and the bat virus RaTG13 was in fact fabricated in order to give the natural evolution theory of SARS-CoV-2 some credence, then the evidence for a man-made pandemic becomes all the more compelling. There's also other evidence that raise serious questions about the origin of this pandemic virus. Other Evidence of ManipulationIn an earlier blog post, dated March 15, 2020, Nerd Has Power explains the importance of the S1 and S2 spikes of a given virus.38 In that post, the blogger also details significant changes found in the S1 portion of the SARS-CoV-2 spike protein, "which dictates which host a coronavirus targets," whereas much of the rest of the spike is very similar to the bat coronaviruses ZC45 and ZXC21. According to the blogger:39
In my opinion, the strongest pieces of evidence so far all point toward SARS-CoV-2 being a laboratory creation. How it got released, however, and why, remains to be determined. The fact that the people responsible would want to cover it up is obvious, however, when you consider that the punishment in such an event could include life in prison for violating the Biological Weapons Anti-Terrorism Act of 1989.40 from http://articles.mercola.com/sites/articles/archive/2020/05/30/wuhan-bio-lab-shut-down.aspx "Why is success in critical care being ignored?" the Alliance for Natural Health rightly asks.1 The organization claims "much more could be done to save lives" if critical care protocols were to take into account what critical care doctors are finding in practice. A May 14, 2020, article reads, in part:2
Front-Line Critical Care Working GroupAs noted by the Alliance for Natural Health, despite the fact that "the obstacle course posed by the peer review process to scientific publication has been removed," and despite many critical care specialists using treatment protocols that differ from standard of care, information about natural therapeutics in particular are still being suppressed by the media and is not received by those who need it most — critical care physicians.
According to the article, efforts by Dr. Pierre Kory — medical director at the Trauma & Life Support Center and a faculty member in the Division of Allergy, Pulmonary and Critical Care Medicine in the Department of Medicine at the University of Wisconsin School of Medicine and Public Health — to share the Front Line COVID-19 Critical Care Working Group's4 (FLCCC) successes with other health care professionals have so far come to naught. Kory was one of five doctors participating in a May 6, 2020, roundtable discussion5 on COVID-19 with ranking senate committee member Gary Peters, D-Mich. In his testimony, Kory states, in part:6
COVID-19 Early Intervention ProtocolAccording to Kory, the FLCCCs MATH+ protocol has been delivered to the White House on four occasions, yet no interest has been shown. Worse, he says they continue to be stonewalled by the U.S. Centers for Disease Control and the National Institute for Health. Why? Isn't saving lives, right now, and by any means possible, more important than pushing for a vaccine? If the MATH+ protocol works with near-100% effectiveness, a vaccine may not even be necessary. The MATH+ protocol gets its name from:
Kory's testimony transcript reviews and summarizes the MATH+ protocol, and explains why the timing of the treatment is so important. As explained by Kory, there are two distinct yet overlapping phases of COVID-19 infection.
The MATH+ ProtocolThe MATH+ protocol7 calls for the use of three medicines, all of which need to be started within six hours of hospital admission:
Optional additions include thiamine, zinc and vitamin D. In addition to these medications, the protocol calls for high-flow nasal oxygen to avoid mechanical ventilation, "which itself damages the lungs and is associated with a mortality rate approaching nearly 90% in some centers," Kory notes.8 Together, this approach addresses the three core pathological processes seen in COVID-19, namely hyperinflammation, hypercoagulability of the blood, and hypoxia (shortness of breath due to low oxygenation). COVID-19 Should Not Be Treated as ARDSIn the video, Dr. Paul Marik points out that it's crucial for doctors to treat each patient as an individual case, as COVID-19 is not conventional acute respiratory distress syndrome (ARDS). If the patient is assumed to have ARDS and placed on a ventilator, you're likely going to damage their lungs. Indeed, research has now shown that patients placed on mechanical ventilation have far higher mortality rates than patients who are not ventilated. While not discussed here, some doctors are also incorporating hyperbaric oxygen treatment in lieu of ventilation, with great success. The reason for this is because the primary problem is inflammation, not fluid in the lungs. So, Marik says, they need anti-inflammatory drugs. "It's not the virus that is hurting the host, it's the acute inflammatory dysregulated response," he says. "That's why you need to use vitamin C and steroids." He points out that steroids play a crucial role, as it creates synergy with vitamin C. COVID-19 patients also have a hypercoagulation problem, so they need anticoagulants. In addition to using the proper medication, they must also be treated early. "You have to intervene early and aggressively to prevent them from deteriorating," Marik says. Methylprednisolone May Be a Crucial ComponentKory expresses concerns over the fact that health organizations around the world are warning doctors against the use of corticosteroids, calling this a "tragic error"9 as "COVID-19 is a steroid-responsive disease."10 In his testimony, he points out:11
As noted by Kory in his senate testimony, Marik, chief of pulmonary and critical care medicine at the Eastern Virginia Medical School in Norfolk, Virginia, is a member of the FLCCC.13 You may recall that Marik was the one who in 2017 announced he had developed an extraordinarily effective treatment against sepsis. Marik's sepsis protocol also calls for intravenous vitamin C and a steroid, in this case hydrocortisone, along with thiamine. I for one am not surprised that the two protocols are so similar, seeing how sepsis is also a major cause of death in severe COVID-19 cases. Safe and Effective Treatments Must Not Be IgnoredAs noted by Marik in the video, COVID-19 is not regular ARDS and should not be treated as such. What kills people with COVID-19 is the inflammation, and steroids in combination with vitamin C work synergistically together to control and regulate that inflammation. The heparin, meanwhile, addresses the hypercoagulation that causes blood clots, which is a unique feature of COVID-19. As for the "lack of studies" supporting their protocol, FLCCC notes:14
I believe this information needs to be shared far and wide, if we are to prevent more people from dying unnecessarily. More and more, as doctors are starting to speak openly about their clinical findings, we're seeing that there are quite a few different ways to tackle this illness without novel antivirals or vaccines, using older, inexpensive and readily available medications that are already known to be safe. from http://articles.mercola.com/sites/articles/archive/2020/05/29/dr-paul-marik-critical-care.aspx As the world’s attention remains focused on the COVID-19 pandemic, essential attention is turned away from other life-threatening epidemics, including opioid addiction. Prior to the COVID-19 crisis, opioid misuse and addiction had become rampant in the U.S. In the late 1990s, drug companies assured doctors that opioid pain relievers were safe and nonaddictive, leading to an increase in prescribing rates. Opioid overdose rates increased rapidly as it became clear that opioids can be highly addictive. In 2018, 46,802 Americans died from an opioid overdose while 1.7 million suffered from substance use disorders related to opioid pain relievers. The economic burden of prescription opioid misuse alone is $78.5 billion in the U.S. annually, which includes not only health care costs but also lost productivity, addiction treatment and criminal justice involvement.1 The economic toll, and the death toll, from the opioid epidemic is, sadly, set to rise even further now that it has collided with the COVID-19 pandemic. COVID-19 Pandemic Heightens Risks for Opioid AddictsThere are physical and psychological reasons why COVID-19 poses a significant challenge for people with opioid use disorder (OUD), which affects at least 2 million Americans, and those who misuse opioids — another 10 million.2 Worldwide, 40.5 million people struggle with opioid dependence, a global prevalence of 510 cases per 100,000 people.3 Chronic respiratory disease increases the risk for fatal overdose in people who use opioids, and COVID-19 leads to compromised lung function. Further, opioid misuse can lead to slowed breathing and hypoxemia, which can cause cardiac, pulmonary and brain complications, as well as overdose and death. As such, according to an article in the Annals of Internal Medicine, “these individuals may be at increased risk for the most adverse consequences of COVID-19.”4 People who are addicted to opioids may also be more likely to suffer from conditions that make them more vulnerable to COVID-19, including being a smoker who suffers from lung or heart disease, being homeless or having experienced other health effects from drug addiction.5 Threat of infection aside, there are a number of indirect ways that people with OUD may be adversely affected by COVID-19 as well. “Before the first COVID-19 case in the United States, a different epidemic — the opioid crisis — was taking the lives of 130 Americans per day,” wrote two doctors from Yale School of Medicine in Annals of Internal Medicine. “Given that infection epidemics disproportionately affect socially marginalized persons with medical and psychiatric comorbid conditions — characteristics of those with opioid use disorder (OUD) — we are gravely concerned that COVID-19 will increase already catastrophic opioid overdose rates.”6 Some of the challenges faced by people with OUD during the COVID-19 pandemic include:7
Disruptions in Care, Increased Anxiety Are ProblematicDisruptions of care during the COVID-19 pandemic are a major concern for people with opioid use disorder, who depend on regular face-to-face health care. Many rehab facilities have closed, limited programs or limited new admissions over fears of COVID-19 spreading in a communal living facility.8 Access to medications for addiction treatment may be restricted, while patients may also face simultaneous challenges like loss of work, housing and food security, which could trigger a downward spiral leading to relapse and delayed recovery. "The COVID-19 pandemic strikes at a moment when our national response to the opioid crisis was beginning to coalesce, with more persons gaining access to treatment and more patients receiving effective medications. COVID-19 threatens to dramatically overshadow and reverse this progress," according to researchers with the Johns Hopkins School of Medicine.9 The social isolation imposed by the pandemic is also highly problematic and, by increasing stress and anxiety, could heighten substance abuse, opioid usage and overdose. In addition to limiting access to peer-support groups and other vital sources of social connection for recovering addicts, “Persons who are isolated and stressed — as much of the population is during a pandemic — frequently turn to substances to alleviate their negative feelings,” wrote Dr. Nora Volkow with the National Institute on Drug Abuse. “Those in recovery will face stresses and heightened urges to use substances and will be at greatly increased risk for relapse.”10 There’s also the issue of social isolation indirectly contributing to overdose deaths because no one is there to administer naloxone, an overdose-reversing drug. Volkow continued:11
There are even reports of stigma and discrimination, according to Dr. Peter Grinspoon, who recovered from opioid addiction and teaches medicine at Harvard Medical School. “There are reports surfacing of police departments across the country that are refusing to offer naloxone to patients who have overdosed, on the pretext that it is too dangerous because the ‘addict’ might wake up coughing and sneezing coronavirus droplets.”12 Job Loss Associated With Opioid Overdose DeathsThe U.S. unemployment rate may skyrocket to 32.1% in the second quarter of 2020, according to the Federal Reserve Bank of St. Louis.13 Previously, the highest rate of unemployment in U.S. history was 24.9%, which occurred in 1933 during the Great Depression.14 The massive job losses may singlehandedly increase opioid overdose deaths, as a strong connection has been revealed between the two in the past. A 2019 study in the Medical Care Research Review journal looked at the effects of state-level economic conditions — unemployment rates, median house prices, median household income, insurance coverage and average hours of weekly work — on drug overdose deaths between 1999 and 2014.15 According to the authors:
An earlier investigation, published in the International Journal of Drug Policy in 2017, also connected economic recessions and unemployment with rises in illegal drug use among adults. Twenty-eight studies published between 1990 and 2015 were included in the review, 17 of which found that the psychological distress associated with economic recessions and unemployment was a significant factor. According to the authors:16
Pandemic May Lead to 75,000 ‘Deaths of Despair’In a report by the Well Being Trust (WBT) and the Robert Graham Center for Policy Studies in Family Medicine and Primary Care, it’s estimated that up to 75,000 people may die during the COVID-19 pandemic from drug or alcohol misuse and suicide. These “deaths of despair” are expected to be exacerbated by three factors already at play:17
In order to come up with their 75,000 figure, the study used data on deaths of despair from 2018 as a baseline, projected levels of unemployment from 2020 to 2029 and then used economic modeling to estimate the additional number of deaths annually. Nine different scenarios were tested, ranging from quick recovery to slow recovery. In the best-case scenario, 27,644 deaths of despair were estimated while in the worst-case example, 154,037 deaths could occur. While 75,000 was deemed to be “most likely,” the researchers noted, “When considering the negative impact of isolation and uncertainty, a higher estimate may be more accurate.”18 “Undeniably policymakers must place a large focus on mitigating the effects of COVID. However, if the country continues to ignore the collateral damage — specifically our nation’s mental health — we will not come out of this stronger,” Benjamin F. Miller, PsyD, chief strategy officer of WBT, said in a news release.19 A commentary by Dr. Jeffrey A. Lieberman, a psychiatrist with Columbia University’s department of psychiatry, similarly suggested a mental health crisis is looming.20 “The sobering reality is that high-quality mental health care is not available to most people,” Lieberman wrote. “This lack of strategy and access is especially concerning amid disasters such as COVID-19, which can cause considerable psychological trauma.” Prolonged Isolation May Lead to Drug AbuseAs mentioned, prolonged isolation only exacerbates the issue. “The stressors from the pandemic are very, very real and how we cope with these stressors varies enormously,” Volkow told ABC News. “Social isolation is one of the factors that leads [people with substance abuse disorder] … to take drugs, and social isolation leads them to relapse, and the social isolation leads them to continue taking them.”21 With weeks of extended isolation already logged for most Americans, some communities are already reporting a rise in drug overdose deaths. Jacksonville, Florida, for instance, had a 20% increase in overdose emergency calls in March 2020. Four counties in New York State also reported a rise in overdoses, while Columbus, Ohio, had a surge in overdose deaths, including 12 over a 24-hour period the first week of April.22 Whether overdose deaths are increasing across the U.S. is unknown, as Volkow noted that with COVID-19 shutdowns, collecting reliable data is difficult. However, a spokesperson for the U.S. Centers for Disease Control and Prevention told ABC News that officials are “aware of the concerns involving COVID-19 and drug overdoses and that it could affect some populations with substance use disorders.”23 Experts are recommending increased resources for people struggling with drug addiction, including access to online meetings. Remember that even if you’re socially isolated at home, you can reach out to friends and loved ones via phone or online. Connecting with others, even virtually, can help you to feel less alone. It’s also a good idea to set a limit on watching the news or browsing social media, especially if it increases anxious feelings.24 from http://articles.mercola.com/sites/articles/archive/2020/05/28/covid-19-pandemic-heightens-risks-for-opioid-addicts.aspx Recent scientific papers have highlighted the role vitamin D may be playing in the COVID-19 pandemic, especially in severe cases. Considering researchers have also shown that SARS-CoV-2 is rapidly inactivated by sunlight,1 areas that are banning people from parks and beaches, are undoubtedly committing a grave error. Social Distancing Is a Miserably Failed ExperimentStay-at-home recommendations in general may also have been a bad idea overall. Indeed, New York Gov. Andrew Cuomo stated,2 May 6, 2020, that 66% of new hospital admissions for COVID-19 were individuals who had been sequestering at home. A majority of those cases were also minorities such as African-Americans, who are far more prone to vitamin D deficiency due to their darker skin.3 When Cuomo first heard about it, he said he immediately thought maybe people had been going out in spite of the shelter-in-place order, and maybe taking public transportation.4 In actuality they were all at home where they were supposed to be. Interestingly, Dr. David Katz, president of True Health Initiative and founding director of the Yale-Griffin Prevention Research Center, predicted5,6 this would happen. Chinese researchers have also noted that a majority of outbreaks in the 320 municipalities reviewed were the result of indoor spread of the disease, with the home accounting for 79.9% of cases, followed by transportation at 34%. According to the authors,7 "All identified outbreaks of three or more cases occurred in an indoor environment, which confirms that sharing indoor space is a major SARS-CoV-2 infection risk." As noted in a May 11, 2020, American Thinker article:8
Banning Outdoor Activities — A Disastrous IdeaIn the video above, published May 11, 2020, on Medscape.com, Dr. JoAnn E. Manson, professor of medicine and chief of the division of preventive medicine at Harvard Medical School, discusses the protective role of vitamin D against COVID-19. Manson points out that growing evidence suggests your vitamin D status may in fact play an important role in your risk of developing COVID-19, as well as the severity of the illness. It's well-known that vitamin D is important for innate immunity and that it boosts your immune function against viral diseases. Importantly, as noted by Manson, vitamin D also has "an immune modulating effect and can lower inflammation, and this may be relevant to the respiratory response during COVID-19 and the cytokine storm that's been demonstrated." Manson cites evidence from three South-Asian studies showing people with serious COVID-19 infection are far more likely to have insufficient levels of vitamin D compared to those with mild illness. Vitamin D deficient patients had, on average, an eightfold higher risk of serious COVID-19 illness compared to those with sufficient levels. Harvard Medical School is starting a study to investigate whether vitamin D supplementation lowers the risk of COVID-19 specifically, and/or improves clinical outcomes, but in the meantime, Manson urges people to spend more time outdoors to improve their vitamin D levels through sun exposure, and to optimize their vitamin D levels through food and supplements. Manson is far from alone in her recommendations. Irish researchers recently published an editorial13 highlighting the role of vitamin D deficiency in severe COVID-19 infections. According to the authors:14
Low Vitamin D Linked to Greater SARS-CoV-2 Infection RiskA May 6, 2020, report15 in the journal Nutrients points out that vitamin D concentrations are lower in patients with positive PCR (polymerase chain reaction) tests for SARS-CoV-2. As noted in this report, which retrospectively investigated the vitamin D levels obtained from a cohort of patients in Switzerland:16
Low Vitamin D Levels Linked to Increased COVID-19 MortalityAnother May 6, 2020, report,17 published in Aging Clinical and Experimental Research (its prepublication featured in the Daily Mail May 118), found that countries with lower vitamin D levels also have higher mortality rates from COVID-19. According to the authors:19
In the preprint version20 of this paper, the authors concluded: "We believe that we can advise vitamin D supplementation to protect against SARS-CoV2 infection." In the final version,21 they toned down the recommendation to: "We hypothesize that vitamin D may play a protective role for COVID-19." GrassrootsHealth StudyData22 from a clinical trial by GrassrootsHealth — an organization that we have supported for over 13 years — also reveals a link between vitamin D status and COVID-19 severity. Mark Alipio — who received no funding for his work — released data from an analysis of 212 people with lab-confirmed COVID-19 and for whom serum 25(OH)D levels were available. Using a classification of symptoms based on previous research, he employed statistical analysis to compare the differences in clinical outcomes against the levels of vitamin D. Of the 212 people, 49 had mild disease; 59 had ordinary disease; 56 were severe and 48 were critical. In the initial study group of 212 patients (see Table 1 below), 55 had normal vitamin D levels, which Alipio defined as greater than 30 ng/ml; 80 had insufficient levels of 21 to 29 ng/ml and 77 had deficient levels of less than 20 ng/ml. 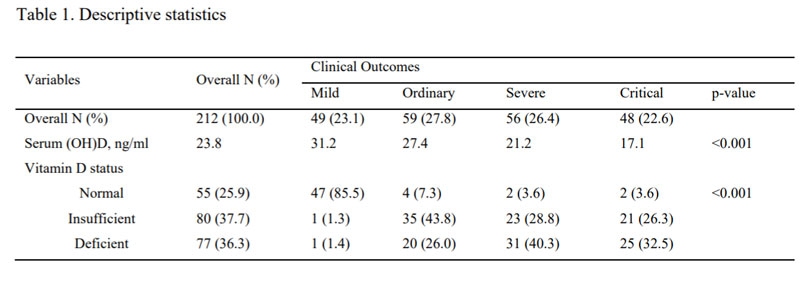
Vitamin D levels were strongly correlated to the severity of the illness experienced. It is important to note that most experts consider 30 ng/ml half of what an optimum vitamin D level should be, which is 60 to 80 ng/ml.
Of the 49 with mild illness, 47 had normal vitamin D levels. For those of you who are not good with math that means that 96% of the patients with mild illness had "normal" levels of vitamin D. Note again this "normal" level was above 30 ng/mL, and most experts would raise that to 60 ng/mL. Of the 104 with severe or critical illness, only four had normal levels of vitamin D. That is 4% or the reciprocal of the mild group. How much stronger a correlation could one hope for? Alipio concluded:23
Vitamin D Protects Against Viral InfectionsIndeed, there is strong scientific evidence vitamin D plays a central role in your immune response and your ability to fight infections in general, so there's little reason to think it wouldn't provide similar protection against COVID-19. In this video, Ivor Cummins, biochemist and chief program officer for Irish Heart Disease Awareness, explains how higher levels of vitamin D may reduce your risk of negative outcomes from COVID-19. He also reviews some of the conditions associated with low vitamin D levels, such as insulin resistance and high levels of inflammation. As discussed in "The Real Pandemic Is Insulin Resistance," obesity, high blood pressure, diabetes and heart disease are comorbidities for severe COVID-19, and insulin resistance is the underlying problem in all of these. As noted in "Vitamin D and the Antiviral State," a literature review article published in the Journal of Clinical Virology in 2011:24
SARS-CoV-2 is an enveloped type of virus,25 which means vitamin D may actually have a direct antiviral effect on it. Future studies will have to confirm that, but in the meantime, there's absolutely no reason to ignore your vitamin D level. As reported in a recent GrassrootsHealth press release:26
from http://articles.mercola.com/sites/articles/archive/2020/05/28/vitamin-d-levels-at-home.aspx Bill Gates has built a global empire around his technologies and “philanthropic” endeavors. His sheer wealth has allowed him to become a veritable superpower in his own right, rising to become the unelected global health tsar on COVID-19. Indeed, the World Health Organization and the White House pandemic response team even kowtows to his nonexistent medical expertise. Life cannot and will not go back to normal until we can vaccinate the entire global population, Gates says, and that same sentiment is being echoed from government leaders and health authorities around the world. Never mind the fact that actual scientists and medical researchers are finding all sorts of simple, inexpensive and safe strategies to address this illness. But vaccinating the global population isn’t enough, in Gates’ eyes. We must also implement surveillance of infection and vaccination status. Not surprisingly, Gates’ recommendations benefit himself most of all. As discussed in “Bill Gates — Most Dangerous Philanthropist in Modern History?” the Bill & Melinda Gates Foundation donates billions to the very same companies and industries that the Foundation owns stocks and bonds in. Using nonprofit money to advance research for companies you're invested in is illegal, yet he’s been getting away with this for many years. At the same time, his Foundation gets tax breaks for the charitable donations it makes money from. Remember, he has “donated” tens of billions, yet his net worth has doubled. This is largely because his “donations” are tax deductible investments. Pandemic Fear-Mongering Pays Off for Tech CompaniesWhile unemployment has reached a historical high during this pandemic, the financial crush is not felt by some. In fact, Gates and other tech billionaires are cashing in big, in a variety of different ways. In a May 8, 2020, article1 in The Intercept, Naomi Klein reports on how New York is tasking Gates with reinventing the state’s “post-Covid reality, with an emphasis on permanently integrating technology into every aspect of civic life.” May 6, 2020, New York Gov. Andrew Cuomo announced the state is partnering with the Bill & Melinda Gates Foundation to develop “a smarter education system” focused on online learning. This, despite the fact that the Common Core curriculum — the Gates Foundation’s previous attempt at remaking American education2 — has been an abysmal failure.3 The state is also partnering with Google, and Cuomo has asked former Google CEO Eric Schmidt to head a new panel to plan the state’s technological infrastructure.4 Schmidt joined Cuomo during a briefing, saying “The first priorities … are focused on telehealth, remote learning and broadband …” As noted by Klein:5
In her article — which is well worth reading in its entirety — Klein reviews how Schmidt and Gates have been working and pushing toward the future that is now staring us square in the face, and how the surveillance apparatus that consumers have been railing against is now being rebranded as the answer to everyone’s health concerns. In a May 6, 2020, article, Vox’s Theodore Schleifer weighed in on Cuomo’s decision to hand over the proverbial keys to the state to tech billionaires whose philanthropy always ends up benefiting themselves the most:6
Schmidt Futures Wants to Make Private Data PublicWhile less visible than Gates, Schmidt can hardly be trusted any more than Gates. Schmidt Futures — Eric and Wendy Schmidt’s philanthropic initiative, which “seeks to improve societal outcomes through the thoughtful development of emerging science and technologies that can benefit humanity”7 — admits that one of its approaches is to “liberate private data with a public purpose.”8 Clearly, infection status falls into a category of private data that is now rebranded as having a “public purpose.” As noted on its website:9
‘Unaccountable Monopolists’ Replace Elected RepresentativesIn a May 14, 2020, Guardian article, Zephyr Teachout and Pat Garofalo comment:10
The Gates, Soros and Clinton Contact Tracing GroupWhether preplanned or not, the COVID-19 pandemic is clearly being used to usher in highly controversial changes that are unmistakably totalitarian-building, including the private take-over of government through public-private partnerships. Contact tracing serves as a convenient bridge12 for this hostile takeover parading as “aid.” Not only is Big Tech offering up contact tracing apps, self-serving billionaires are also funding contact tracing groups that will provide “boots on the ground” services. For example, Partners in Health — the group selected by Massachusetts Gov. Charlie Baker to conduct COVID-19 contact tracing using teams of investigators to interview people who test positive — is funded by Gates and one of the richest men in the world, George Soros. The William J. Clinton Foundation has also funded Partners in Health in the past.13 Chelsey Clinton sits on its board of trustees, and one of the group’s co-founders, Jim Kim, spent three years at the WHO14 and is currently the president of the World Bank. He rejoined Partners in Health’s board of directors in January 2019.15 UK Demands Answers About COVID Data DealMeanwhile, on the other side of the pond, OpenDemocracy and the tech start-up Foxglove are demanding the U.K. government share the details of its patient data deals with Big Tech. In a May 7, 2020, post, OpenDemocracy.net writes:16
While the amount of British health data being shared with these companies has been described as “unprecedented,” the U.K. government has yet to release the details about the partnership. Suspiciously, Palantir is reportedly providing its COVID-19 Datastore services to the NHS for just £1.18 This despite the fact that its services are estimated to cost around £88,000 a week, and that’s just for salaries.19 How and why is Palantir giving away its services for free? The old adage, “There’s no such thing as a free lunch” seems applicable here. OpenDemocracy also questions how the artificial intelligence (AI) startup Faculty has managed to land seven different government contracts worth nearly £1 million in the last 18 months.20
UK Government Ignores FOIA RequestFoxglove submitted Freedom of Information Act (FOIA) requests to the U.K. government on April 3, 2020. A reply is required within 20 working days, yet no response has been forthcoming. The British Information Commissioner’s Office, the independent regulator responsible for FOIA enforcement, has announced21 it has relaxed enforcement for the duration of the pandemic crisis. That seems suspiciously convenient, considering deals are being made in secret that shouldn’t be, and panic is being drummed up without much real-world data to support the narrative that we’re still in a high-risk situation.22
Tech Initiative Seeks to Alter Global BehaviorAnyone still living under the misguided spell that governments’ responses to this pandemic are simply temporary emergency measures need to rapidly reassess. As reported by Vox,23 tech billionaires like Gates and Schmidt are hard at work trying to convince governments and the public at large that only they can save us from another pandemic. Such is the focus of the Pandemic Action Network, responsible for the #MaskingForAFriend Twitter campaign, pushed by Hillary Clinton and other celebrities.24
Digital Health Passports Coming to 15 NationsA lead-in to global totalitarianism, predicated on protecting public health and preventing another pandemic, is the issuance of “digital health passports.” According to the British tech magazine Verdict,25 coronavirus digital health passports are now being supplied to 15 nations. The passport is “designed to make it easier for individuals to return to work after the Covid-19 coronavirus pandemic” — as if we’ve never been able to return to normal life after any other epidemic or pandemic scare. In a May 11, 2020, article Verdict reports:26
According to Covipass.com,28 the app will display “your COVID-19 test history and immunoresponse and other relevant health information.” As I’ve stated before, a RT-PCR (reverse transcription polymerase chain reaction) test result is basically worthless, since a) it merely detects the presence of SARS-CoV-2 genetic material, not the actual virus, and b) you can get infected at any time after you get your test results, rendering the “verification” of your infection status null and void. According to a recent speech by U.S. President Donald Trump, his administration is mobilizing the military to distribute the vaccine once ready, which could be as early as the end of 2020. At the same time, the U.S. Senate has voted to renew federal surveillance powers that would otherwise have expired,29 and an ill-named bill, HR 6666, would put the government in charge of COVID-19 tracking and tracing, costing taxpayers a whopping $100 billion.30 Virus Surveillance and Civil Liberties CollideAs predicted in a Law360 article31 published April 26, 2020, virus surveillance is now colliding head-on with civil liberties:
The answer to that question should be a resounding “no.” The idea that government can keep you safe against a virus by giving up your civil liberties is a fantasy that must be outgrown. As noted by CNN Business:32
It’s time to fully recognize that surveillance has become the biggest for-profit industry on the planet, and your entire existence is now being targeted for profit. For a better understanding of what you’re giving up by going along with the mainstream narrative that we need Big Tech to save us, see my article about social psychologist and Harvard professor Shoshana Zuboff and her extraordinary book, "The Age of Surveillance Capitalism." from http://articles.mercola.com/sites/articles/archive/2020/05/27/tech-companies-coronavirus.aspx |
Nia Pure NatureThe Provider of premium Quality Health Products To Live Better Lives Archives
March 2022
Categories |
 RSS Feed
RSS Feed
