|
I’ve previously reviewed the similarities between the flavonoid quercetin and the drug hydroxychloroquine, discussing the possibility of using quercetin in lieu of the drug against COVID-19. We’re now also starting to see quercetin mentioned more often in the scientific literature on COVID-19. Quercetin Highlighted in COVID-19 Medical LiteratureFor example, a review article1 published in the June 19, 2020, issue of Frontiers in Immunology highlights quercetin’s usefulness as a COVID-19 treatment, especially in conjunction with vitamin C. Quercetin is also featured in a review2 of emerging COVID-19 research published in the Integrative Medicine journal. As reported by MedPage Today:3
Why Quercetin May Offer Hope Against COVID-19There are solid reasons to suspect quercetin can be effective against SARS-CoV-2, the virus that causes COVID-19 disease. For example, quercetin has been shown to:
Quercetin Studied as COVID-19 Treatment and ProphylaxisAs reported by MedPage Today,24 Dr. Hasan Önal is currently conducting an open-label nonrandomized trial25 on quercetin in Turkey. COVID-19 patients are given 1,000 milligram (mg) of quercetin per day as an active treatment, while front-line health care workers are receiving 500-mg doses as a prophylaxis. As noted by the researchers:26
Vitamin C Enhances Quercetin’s EfficacyVitamin C has been shown to enhance plasma quercetin levels,27,28 and the duo is the subject of the Frontiers in Immunology review article,29 “Quercetin and Vitamin C: An Experimental, Synergistic Therapy for the Prevention and Treatment of SARS-CoV-2 Related Disease (COVID-19),” mentioned earlier. That review, by the way, was co-written by Dr. Paul Marik, who in 2017 discovered a highly effective vitamin C-based sepsis treatment. In “Quercetin and Vitamin C,” Marik and co-authors point out that:30
Vitamin C and Quercetin Both Provide Antiviral ProtectionIn summary, aside from having direct viricidal effects, vitamin C:31
All of these effects contribute to vitamin C’s antiviral effects. Like vitamin C, quercetin also has antioxidant, anti-inflammatory, antiviral, immunoprotective and immunomodulatory properties. According to Marik’s review paper, many of quercetin’s antiviral effects are attributable to its inhibition of:32
Quercetin also inhibits platelet aggregation,33 which is pertinent with regard to COVID-19, seeing how many patients suffer abnormal blood clotting. It also has powerful anti-inflammatory effects, inhibiting lipid peroxidation and proinflammatory mediators.34 Quercetin and Vitamin C Work SynergisticallyMarik’s paper goes on to explain the synergistic antiviral action of the two compounds together:35
Optimal DosingAccording to “Quercetin and Vitamin C,”36 both vitamin C and quercetin have excellent safety profiles, and oral supplementation with quercetin at doses up to 1 gram (1,000 mg) per day for three months has not resulted in any significant side effects. “Only higher intravenously administered doses up to 51.3 mg/Kg (around 3,591 mg per individual) were associated with renal toxicity,” the paper notes. The following table shows the proposed dosages for concurrent use of vitamin C and quercetin, either as a prophylactic for high-risk groups, and/or treatment for mild to severe COVID-19 disease. 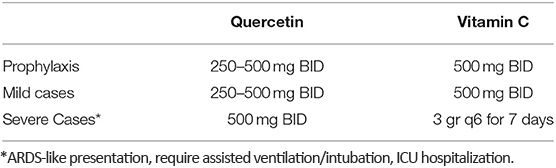
The Importance of ZincWhile Marik’s paper does not address the use of zinc, it seems reasonable to recommend oral zinc supplementation as well, especially if you’re older. In fact, two oft-noted early symptoms of COVID-19 — the loss of taste and smell — are both symptoms of zinc deficiency. As noted in the Integrative Medicine journal’s review37 of emerging COVID-19 research, “Zinc plays a crucial role in the function of essentially all immune cells,” and “Deficiency of this critical element has a profound impact on immune response, increasing susceptibility to a variety of infections.” Like quercetin and vitamin C, zinc also has well-known antiviral properties in its own right. As noted in the Integrative Medicine journal’s review:38
My Personal Take on This and Strong RecommendationsI am a huge fan of zinc, quercetin and vitamin C, but it is important to understand some very basic principles before using them. It is clear in my mind that quercetin is far less expensive, is safer and is likely equally effective to hydroxychloroquine at driving zinc into the cell, where it does its job of inhibiting viral replication, and unlike hydroxychloroquine, it reduces inflammatory cytokines and also increases interferon. However, it is important to understand that if this excellent strategy is going to be optimally effective it needs to be administered early in the disease phase — the earlier the better. Using quercetin and zinc would be best done if you were recently exposed to the virus. This way you can inhibit viral replication and keep the viral load low while your innate immune system does its work in clearing the virus. With respect to vitamin C, it is my perception that there is major confusion in this area. It can be used in low doses of several hundred milligrams to meet nutritional requirements and support your immune system in the early phase of the illness. However, if you’re really sick and have shortness of breath, and are considering being hospitalized or are already in the hospital, then you need very high doses of vitamin C in the 10 gram to 100 gram-dose per day, either through liposomal or IV administration. I don’t recommend taking high doses of vitamin C unless you are acutely sick. The bulk of the literature reviewed here is promoting the use of vitamin C to regenerate quercetin, but I believe there are far more powerful approaches. What might that be? It seems obvious to me that quercetin is best taken at night (with zinc) before you go to bed and you haven’t eaten for at least three to four hours. You will sleep for eight hours, and if you are metabolically flexible, this is the time that you will dive into nutritional ketosis. Ketosis will increase your NADPH levels, which is FAR superior to vitamin C at recycling antioxidants like quercetin. The other benefit of taking quercetin at night is to take advantage of its senolytic action to remove senescent cells, which are similar to nonreplicating cancer cells that secrete powerful proinflammatory cytokines that destroy your health. You can optimize quercetin’s senolytic properties if you take it while you are fasting. from http://articles.mercola.com/sites/articles/archive/2020/07/24/coronavirus-prevention-quercetin.aspx
0 Comments
The global pandemic has spurred several arms of science into action, with researchers seeking to discover how the virus works and to uncover the best testing, vaccinations and treatments. The biomedical community has been working on antiviral interventions, including remdesivir. A precursor to the drug was initially evaluated during the Ebola outbreak several years ago. Remdesivir was developed using taxpayer money that Public Citizen estimates reached at least $70.5 million, based on publicly available data.1 They also believe the number is likely higher. A 2017 report noted that the Department of Defense “is cost sharing with Gilead Biosciences for continued development of this product.”2 At the time it was labeled GS-5734.3 Public Citizen reports the DOD granted Gilead Biosciences $34.5 million.4 Additionally, the NIH led the Ebola trials using remdesivir, which opened the door for research into the use with COVID-19. The NIH granted nearly $700 million to groups for coronavirus research, including $6 million to the University of North Carolina to move the development of the drug forward. Despite the large amount of taxpayer money poured into research and development from sources other than itself, the company has set a price of more than $3,100 for a single course of treatment.5 While most see this as one example of how Big Pharma is again fleecing the public, NPR justified the pricing process by commenting that the price was determined only: “after months of speculation as the company tried to figure out how to balance profit and public health needs in the middle of a pandemic.” Gilead claims this to be a fair price that will give everyone access:6
Remdesivir Lowers Viral Load at an Enormous Health CostYet, this curiously high price tag is on a drug that has not produced adequate results and has not been proven to reduce the potential for death in those with severe disease. Worse, the so-called “clear-cut, significant, positive effect in diminishing the time to recovery”7 of remdesivir with COVID-19 comes with an additional price tag that may include renal failure requiring a kidney transplant. In a paper published in the International Journal of Infectious Diseases, scientists reported on five of the first patients treated in France with remdesivir.8 French authorities allowed for the “compassionate-use” treatment of the drug, which is still being studied. In the paper, the authors describe the outcome for the first five patients admitted with severe pneumonia to the University Hospital of Bichat, Paris, France. Following the administration and encouraging results of a recent clinical study and two case reports, five patients admitted to the hospital were treated with the drug. Criteria included signs of severe illness and clinical aggravation of a patient's symptoms. All patients received a loading dose of 200 mg and a planned daily maintenance of 100 mg for 14 days, unless the drug was otherwise stopped for side effects. The team also collected nasopharyngeal and lung samples, which were tested for viral and bacterial growth. These were the results: • Case 1 -- A 31-year-old man from Wuhan, China, started on the drug on illness Day 11. It was stopped four days later because of liver alterations and a maculopapular rash. The liver abnormalities improved after discontinuing the treatment. • Case 2 -- An 80-year-old man from China was given remdesivir for two days. It was discontinued when his kidneys failed. The gentleman received the drug again as the disease severity persisted and progressed. He died nine days later. • Case 3 -- A 39-year-old man with obesity and obstructive sleep apnea received eight doses of remdesivir, which was stopped because of liver enzyme alterations and the same kind of rash as was seen in Case 1. This resolved after the drug was discontinued. The gentleman was discharged on day 20. • Case 4 -- A 76-year-old man from France with a history of chronic kidney injury received remdesivir for nine days without side effects. He was discharged on illness day 23. • Case 5 -- A 70-year-old man with a history of chronic obstructive bronchopneumopathy was admitted with acute respiratory distress syndrome. Remdesivir was given for two days and discontinued because he suffered acute kidney injury, requiring a kidney transplant. His disease progressed and he died. The team recorded four of the five patients with major side effects, including kidney failure that would have required a transplant had the patients lived. A second study included 53 patients who were also treated under the compassionate use, funded by Gilead Sciences.9 The company recorded 36, or 68%, demonstrated clinical improvement. This was measured by improvement in oxygen transport, extubation from mechanical ventilation or discharge. During the study period, although 36 showed clinical improvement, only 25 were discharged. As an added note, the authors of the International Journal of Infectious Diseases studies10 mentioned that they had “waived the need for informed consent from individual patients” — which implies that the patients had no idea they were being given an experimental drug. Also intriguing is that the authors casually noted that “12% of the patients in the remdesivir group discontinued remdesivir due to adverse events, versus 5% in the placebo group.” In other words, more than twice as many patients in the remdesivir group stopped their treatments due to adverse events than those receiving placebos. The authors ended with the comment, “A particular attention should be given to hepatic and kidney function when administrating this treatment.” NIH Treatment Guidelines Produced by Experts?The NIH brought together a panel of experts, including doctors and statisticians, to develop guidelines to treat coronavirus in the U.S.11 The guidelines are intended to be based on published, peer-reviewed data and to incorporate preliminary data from pre-published studies and the panelists’ clinical expertise. The panel is charged with looking at two categories of therapies. The first are antivirals intended to target the virus directly. The second are immune-based options and host modifiers, which affect the natural immune response. The panel's conclusions are published online at a website supported by the NIH, which is considered a living document intended for information from panel discussions and conclusions, including clinical data and ongoing trials for therapies.12 The members of this highly influential panel had to disclose financial conflicts they may have.13 Those disclosures are published by the NIH and reveal interesting information. There are 53 experts on the panel, eight of whom declared financial benefits from research support or consulting fees originating from Gilead Biosciences, the manufacturer of remdesivir. However, the links to pharmaceutical and biotech companies whose bottom lines are impacted by the pandemic don’t stop there. In the group, 40 did not declare any financial support, while 13 did. All 13 had ties to at least one pharmaceutical, while three had ties to three or more companies. The various types of businesses included biotechnology organizations, a blood research laboratory and a flu vaccine company. The types of jobs that garnered the financial support included:
Remdesivir Studies Lack Positive ResultsAlthough Gilead Biosciences continues to move forward in their distribution of remdesivir, the scientific evidence has not supported its use. In this video, Del Bigtree from Highwire Talk and CEO of Informed Consent Action Network, outlines the problems with three published studies evaluating the effectiveness of the drug. In one study published in the New England Journal of Medicine, the scientists changed the end point measurements for the study,14 moving all to secondary outcome measures except the number of days to recovery, which was the single primary outcome measure at the conclusion of the study.15 The trial was also funded by the National Institute of Allergy and Infectious Diseases (NIAID), of which Dr. Anthony Fauci is director.16 There were significant problems with the research design, and consequently the data, that I discuss in “The New COVID-19 Medication Isn't Backed by Results.” The release of the study generated enthusiasm and triggered immediate action across many countries, including the U.S. The U.S. Food and Drug Administration issued an emergency use authorization on May 1, 2020, since the drug had not yet been approved for use in the U.S. This opened the door for compassionate use of the drug. In the statement the FDA said:17
One team evaluated the use of the drug in those with severe disease enrolling patients who were 18 years and older with lab-confirmed infection. The study was published in The Lancet and concluded the drug was “not associated with statistically significant clinical benefits.”18 The links between the NIH, Fauci and Gilead Biosciences is a demonstration of the importance of financial ties in scientific research and the development of public policy. As mentioned above, the NIH, NIAID, Department of Defense, and countries around the world funded the study published in the New England Journal of Medicine, essentially declaring remdesivir a success. When you consider that Fauci, by virtue of being NIAID’s director, has a vested interest in the development of remdesivir, and that it was he who declared the results to be "highly significant,” it certainly suggests that he, too, should be declaring a conflict of interest in remdesivir’s fate.19 When he was asked about the results of the study published in The Lancet, which had to be stopped because of serious adverse events, Fauci disregarded the evidence as "not adequate." Health Choices That Make a DifferenceSome health experts and the media are crying out over the number of new cases of COVID-19 being diagnosed each day, encouraging citizens to stay in place and wait for a vaccination. However, I recommend that you proactively work to support your immune system in ways that research has demonstrated reduce your risk of severe disease. You can find a number of simple, yet significant strategies on my Coronavirus Resource Page, including proper hand-washing, getting adequate sleep and staying hydrated. However, it has become more apparent with every passing week that optimizing your vitamin D level will be the easiest, least expensive and most beneficial strategy you can use to minimize the risk of severe disease. Health authorities have been warning of a second wave of the disease that is expected in the fall. This means the best time to start addressing your vitamin D level is right now. You can read more about the importance of Vitamin D and how the body uses it to combat coronavirus and other infectious diseases in “The Most Important Paper Dr. Mercola Has Ever Written.” It is my hope that you spread the word about the significance of this to your friends and family. An important part of the strategy is to share the information with influencers in the Black community, as this group historically as had low levels of vitamin D — therefore putting them at greater risk of acquiring the coronavirus. People in nursing homes and skilled nursing facilities, along with the elderly also have notoriously low levels of vitamin D that put them at greater risk of severe COVID-19 and flu, as well. Within my report I go into detail about how to raise your levels between 60 ng/mL and 80 ng/mL by fall. You'll find a quick summary of the key steps in the article linked above including how to get tested, why you should get tested and how to assess your individualized vitamin D dose to raise your level. With this data you can help significantly reduce your risk of severe disease. from http://articles.mercola.com/sites/articles/archive/2020/07/24/remdesivir-side-effects.aspx According to the American Academy of Pediatrics (AAP), the academic, physical and mental benefits of returning children to school for in-person learning outweigh the potential health risks of COVID-19. To that end, the AAP has issued guidelines for the “safe reopening” of schools. However, many parents wonder whether the guidelines themselves may do far more harm than good in the long term. One parent outlines her concerns in the video above. The U.S. Centers for Disease Control and Prevention has also issued school reopening guidelines1 in anticipation of nationwide reopenings. Unicef2 also supports students’ re-entry into schools, noting that reopenings should “be consistent with each country’s overall COVID-19 health response to protect students, staff, teachers and their families.” American Academy of Pediatrics Calls for School ReopeningsAs noted in the AAP’s guidance for school re-entry:3,4
Children Rarely Transmit COVID-19AAP points out that, unlike the influenza virus, SARS-CoV-2 does not appear to spread easily among children and teens. Indeed, studies from the U.S.,5 Israel6 and the Netherlands7 have demonstrated that children are far less likely to become infected than adults, and far less likely than adults to transmit the virus to others. In one such study,8 children accounted for just 13% of transmissions within households. Another found9 children under the age of 4 were 47% less likely to test positive for SARS-CoV-2 infection compared to adults in the same household. A July 2020 study10 looking at COVID-19 in children and the dynamics of infection within families found only 0.9% of COVID-19-positive patients were under the age of 16, and in just 8% of cases did a child within the household develop symptoms before an adult. Science Daily11 also cites a number of other studies confirming the theory that children are rare disease vectors when it comes to COVID-19:
Originally, school closings were based on the premise that the virus responsible for COVID-19 would behave like other respiratory viruses, but since it doesn’t, returning children to school is unlikely to pose a significant risk to health.
Guidelines Promote ‘Institutionalized Isolation’As mentioned, the CDC has also issued guidelines13 for the re-opening of schools. While the CDC and AAP guidelines are very similar, the AAP’s restrictions tend to be a bit more flexible. For example, while both call for social distancing with 6 feet between each student at all times, the AAP concedes that this may not always be feasible, and if not, spacing can be 3 feet if students wear face masks and are asymptomatic. Still, as noted in the featured video, students are likely to be just as scarred having to follow COVID-19 prevention guidelines as they are staying at home. While the exact measures vary depending on the age of the students, some of the basic recommendations found in the CDC and AAP guidelines include:14,15,16,17
As noted in the featured video, these guidelines amount to “institutionalized isolation” and fear-mongering that can cause significant emotional and mental harm to children, especially if implemented for weeks or months on end. Humans need physical contact and social face-to-face interactions, and this is particularly true for children. At best, these remedies will lead to the creation of a generation of fearful germophobes. At worst, it may stunt their ability to function normally in social situations altogether. Choices Vary Depending on Where You LiveWhile the AAP and CDC are calling for the reopening of most schools nationwide, parents may face a variety of choices, depending on where they live. As reported by USA Today:18
In a June 12, 2020, article19,20 in The New York Times, epidemiologists weighed in on the decision to send children back to school. Of the 304 epidemiologists that replied to the New York Times’ survey, a majority — 70% — said they were ready to send their children back to school somewhere between now and this fall. 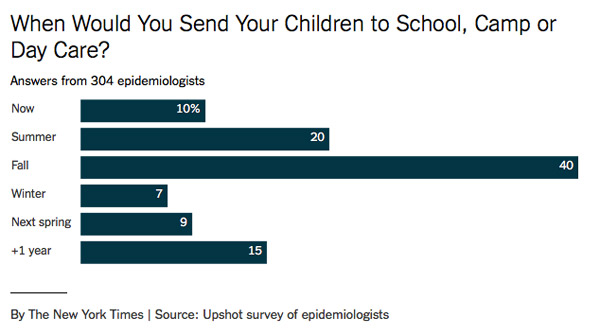
Costs May Have Catastrophic Consequences for School SystemsOn top of everything else, there are financial dilemmas to address. As noted in a July 9, 2020, New York Times article,21,22 school budgets that are already stretched thin are facing million-dollar expenditures if they are to comply with school opening guidelines:
As reported by U.S. News,23 some school systems are already feeling the economic pain from the shutdown. Both state and local budget cuts are expected in many areas, some projected to be as high as 25%, due to lost revenue. In Massachusetts, 2,000 teachers have already been laid off due to budget cuts, and the National Education Association estimates upward of 700,000 teachers may lose their jobs over the next two years. Some states are also seeing skyrocketing homeschooling submissions, which further threatens schools’ funding. In North Carolina, the online system for filing a Notice of Intent to Establish a Home School temporarily crashed24 due to the influx of NOIs being filed, according to a July 7, 2020, report by Life Site.25 I personally find this very encouraging as most educational systems in the U.S. leave much to be desired. While it certainly is an additional challenge for parents, I am convinced most children will be far better off home schooled. Mask Test Reveals Hazardous Carbon Dioxide LevelsLast but certainly not least, many parents worry the wearing of face masks might jeopardize the health of their child by restricting oxygen flow and allowing for the buildup of carbon dioxide with each exhale. There may indeed be something to this concern, and it’s something that none of the health authorities have addressed. The Occupational Safety and Health Administration (OSHA), which is part of the U.S. Department of Labor, requires the oxygen level in a working atmosphere to be above 19.5%. Anything below that is considered hazardous to health. In the video above, which, of course, was banned and removed from YouTube, Del Bigtree shows a video of a man demonstrating how the oxygen concentration — when wearing a surgical mask — can easily drop below OSHA air quality standards. Bigtree then conducts a simple carbon dioxide test with his 11-year-old son to check the air quality behind a variety of masks.26 Using a testing device that measures carbon dioxide concentrations in ambient air, Bigtree checks the carbon dioxide concentration behind his son’s mask. With an N95 mask on, the carbon dioxide level spikes above 8,480 parts per million (ppm) within seconds. Above 5,000 ppm, OSHA warns that “toxicity or oxygen deprivation could occur.” Carbon dioxide levels between 2,000 ppm and 5,000 ppm are associated with headaches, sleepiness, poor concentration, loss of attention, increased heart rate and slight nausea. The maximum permissible daily exposure limit is 5,000 ppm. Wearing a standard surgical mask, carbon dioxide levels again reached above 8,000 ppm, although it took longer. Shockingly, wearing a cloth bandana resulted in carbon dioxide buildup near the nose and mouth exceeding 8,000 ppm. Even wearing a clear plastic face shield (without a mask) resulted in carbon dioxide levels in the 1,500-ppm range, which is associated with drowsiness and poor air quality. There Is No Scientific Basis for Most of These MeasuresUnfortunately, many have been swept up in the mainstream media fearmongering that has bombarded us daily for several months, and when government and health officials encourage shaming and reporting those who refuse to succumb to irrationality, it only worsens matters. The scientific evidence is clear on several points, however. We now know children are not significant vectors of disease, even when they’re infected. Children are also at virtually zero risk of death when they develop symptoms. Even among adults, the infection mortality rate is now down to a median of about 0.25%.27 As Stanford University's disease prevention chairman Dr. John Ioannidis noted in a June 27, 2020, interview with Greek Reporter:28,29,30
And, as testing continues, and more people are found to be asymptomatic yet positive, these mortality rates will be driven down even further. Science also conclusively shows that masks do not protect the wearer against viral infection and do not prevent its spread to others. This evidence was clearly laid out in my interview with Denis Rancourt, Ph.D. He did a comprehensive review of the scientific literature on masks, concentrating on evidence showing masks can reduce infection risk, especially viral respiratory diseases:
Third, we also now know that COVID-19 has not been the devastating pandemic killer it’s been made out to be. When looking at all-cause mortality from year to year, Rancourt found the pandemic has not led to a significant increase in deaths compared to the same time frame in previous years. To understand why all-cause mortality statistics are crucial for understanding the impact of this pandemic, please review my interview with Rancourt. Clearly, I’m not going to tell you what to do with your children. The choice to send your children back to school will have to be a personal one. All I will suggest is to look at some of the statistics and scientific evidence brought forth in this article. Look up the references, read the studies. Try to really understand the data. Chances are, armed with science rather than mainstream media reports, you’ll be better equipped to make your choice, and feel confident in doing so. from http://articles.mercola.com/sites/articles/archive/2020/07/23/school-guidelines-coronavirus.aspx During the COVID-19 pandemic, legitimate concerns have been raised that the social distancing, financial upheaval, quarantines and virus fears could lead to an upcoming mental health crisis. While this is still a potential reality, challenging times bring out both the best and the worst in people, and there’s some evidence that there could be a silver lining to the pandemic, in the form of increased resiliency and fortitude. Rather than leading to an increase in feelings of loneliness, at least one study has found that the unique circumstances surrounding the pandemic, including stay-at-home orders, led to increased feelings of social support among survey respondents.1 Increased Resilience, Social Support During PandemicFlorida State University (FSU) College of Medicine researchers surveyed 2,230 people to assess the trajectory of loneliness in response to COVID-19. While it was expected that loneliness levels would increase, this wasn’t what the study revealed. Loneliness was assessed before the outbreak, in January and early February 2020, in late March when the U.S. was just starting its “Slow the Spread” campaign, and again in late April, when most states had enacted stay-at-home orders.2 “Contrary to expectations, there were no significant mean-level changes in loneliness across the three assessments,” the researchers wrote, and the study suggests people may be finding creative ways to stay connected, and perhaps are calling their friends and family more often than they would have otherwise, during the pandemic. Rather than finding survey respondents to be increasingly lonely as the pandemic wore on, they reported a perception of increased support from others. There were some differences by age, with older adults reporting less loneliness overall, but an increase in loneliness during the outbreak’s acute phase. This leveled off after stay-at-home-orders were issued. Other potentially vulnerable populations, including those living alone or with at least one chronic health condition, did have higher levels of loneliness at the start of the study, but the levels did not increase along with social distancing measures. “Despite some detrimental impact on vulnerable individuals, in the present sample, there was no large increase in loneliness but remarkable resilience in response to COVID-19,” the researchers explained.3 “There has been a lot of worry that loneliness would increase dramatically because of the social distancing guidelines and restrictions,” lead study author Martina Luchetti, an assistant professor at the College of Medicine, said in a news release. “Contrary to this fear, we found that overall loneliness did not increase. Instead, people felt more supported by others than before the pandemic. Even while physically isolated, the feeling of increased social support and of being in this together may help limit increases in loneliness.”4 Other Research Has Hinted at Soaring Stress LevelsWhile it’s possible that challenging times may bring out newfound resilience in many people, other research reveals Americans are struggling with soaring stress levels amid the pandemic. For instance, the American Psychological Association’s Stress in America 2020 survey, released in May 2020 and conducted in partnership with The Harris Poll, found high stress levels related to coronavirus are “the new normal” for parents, while people of color were also more likely than white adults to report that the pandemic was causing significant stressors in their life, particularly related to fears of getting COVID-19 and having access to basic needs and health care services.5 A poll conducted by the American Psychiatric Association in March 2020 revealed that 36% of Americans felt coronavirus was having a serious impact on their mental health, while 59% felt it was seriously impacting their day-to-day lives.6 Even Small Increases in Loneliness MatterIn regard to loneliness, even small, population-wide increases in feeling lonely could have a significant effect on public health, considering loneliness’ toll on your health is equivalent to smoking 15 cigarettes a day7 and increases your risk of premature death.8 Loneliness was even associated with a 40% increased risk of dementia over a 10-year study period.9 Pre-pandemic, in a survey of 20,000 U.S. adults, 46% said they sometimes or always feel alone.10 “In the context of the coronavirus pandemic, it may be particularly difficult to reconnect with others given the restrictions on in-person social gatherings,” Luchetti says. “Even these transient feelings of loneliness can have a negative effect on health, meaning there could be dangerous unintended consequences if loneliness increases in response to the restrictive measures taken as a result of the pandemic.”11 While it seems counterintuitive that the pandemic may have led to increases in perceived social support, it’s possible that the global experience has been unifying. “Just knowing that you are not alone and that everyone is going through the same restrictions and difficulties may be enough in the short term to keep feelings of loneliness down,” Angelina Sutin, FSU associate professor of behavioral sciences and social medicine and senior author of the featured study, said in a news release.12 Becoming ‘Antifragile’ During the PandemicIt’s important to note that there are multiple ways to harness a challenging time like a pandemic to make yourself increasingly resilient or, as Siim Land, whom I recently interviewed, puts it, “antifragile.” His latest book, “Stronger by Stress: Adapt to Beneficial Stressors to Improve Your Health and Strengthen the Body,” reviews the important concepts of hormesis and antifragility.
Time-restricted eating is one of Land’s favorite tools because it allows you to become metabolically flexible and insulin sensitive, which builds your antifragility. However, there are other methods for staying resilient during the pandemic as well. Resilience Sends You on an ‘Upward Spiral’Resilience is the ability to quickly recover from difficulties. It’s an innate toughness that allows you to persevere through challenging times, and it’s something often found among centenarians. Even as times changed, those in the 100-plus crowd kept on living, adapting to and welcoming the new phases of their lives. It’s this fortitude and emotional resilience that has likely played a major role in their longevity — and it’s something you can harness as well, including during the pandemic. Researchers with the University of North Carolina at Chapel Hill’s Positive Emotions and Psychophysiology (PEP) Lab have been looking into what’s making people happy and resilient, despite the pandemic. They note:13
Keys to Staying ResilientAfter surveying more than 600 U.S. adults about their experiences and behaviors of the past day, some clear trends were revealed. Positive emotions were associated with self-care, such as engaging in a hobby or relaxing, exercising or engaging in spiritual activities, such as prayer or meditation.14 This isn’t entirely surprising, but an important finding was that people who were feeling the most stressed, lonely or anxious benefited the most from these positive, self-care activities. This reiterates how important it is to take time to unwind, especially if you feel you’re nearing burnout. Spending time actively engaging with others also led to more positive emotions, and this was true for both introverts and extroverts and was especially beneficial for people who live alone. However, the most positive emotions were gleaned from face-to-face, voice or video interactions — texts didn’t seem to do the trick, with the researchers explaining:15
Passively browsing social media, such as scrolling through feeds, did not lead to positive emotions and instead was strongly tied to negative feelings and anxiety. On the other hand, doing good for others was associated with positive feelings — a finding that’s been proven in the past.16 To sum up their data, the PEP Lab researchers suggested the media stop touting the need for “social distancing,” when what’s really needed is physical distancing combined with social solidarity. In order to retain and find your resilience during the pandemic, increased connections are key, and they suggested the following five steps to help society “MARCH” together:
To help you accept and release negative emotions, the Emotional Freedom Techniques (EFT) is another recommended tool for coping with COVID. from http://articles.mercola.com/sites/articles/archive/2020/07/23/silver-lining-of-pandemic.aspx Up to 7.8% of the U.S. adult population takes proton pump inhibitors (PPIs), medications that are prescribed for acid-related disorders like heartburn, gastroesophageal reflux (GERD) and chronic indigestion.1 For years, the aggressively advertised medications have been a lucrative Big Pharma venture, but they’re also controversial because they are linked to many health risks. PPIs have been overprescribed, wrongly prescribed and over-advertised. For example, 46% to 63% of patients seen in ambulatory care settings who were taking PPIs had no gastrointestinal (GI) complaint or "documented indication for anti-secretory therapy," according to an article in Clinical Correlations, the NYU Langone Online Journal of Medicine.2 They are also routinely used in intensive care unit (ICU) settings.3 Though PPIs were designed to be taken for no more than eight weeks when first approved by the FDA, they are often used long-term despite their well-documented risks.4 According to Clinical Correlations, PPIs:5
Further, PPIs are habit-forming and difficult to quit. Now, scientists writing in the American Journal of Gastroenterology have added another layer to the recognized risks of these drugs: They have found links between taking PPIs and the risk of developing COVID-19.6 Increased Risk of COVID-19 Seen With PPI UseIn the study, of 86,602 eligible survey respondents, 53,130 (61.3%) listed "prior abdominal pain or discomfort, acid reflux, heartburn or regurgitation" on their surveys. They were asked about their use of PPIs and H2 receptor antagonist (H2RA) drugs, which are also prescribed for acid-related disorders.7 Of that group, 3,386 (6.4%) participants reported that they had tested positive for COVID-19.8 Upon analyzing the data, the researchers found that people taking PPIs once a day had more than two times the risk of contracting COVID-19 than those who didn’t.9 For people taking PPIs twice a day, it was even worse: They had more than three times the risk of contracting COVID-19 than those not on the drugs.10 People on H2RAs did not have an elevated risk.11 To rule out confounding data, people who had taken PPIs for less than a month, possibly for COVID-19-like symptoms, were classified as nonusers.12 In their analysis, the study’s authors did not find that taking PPIs increased the odds for reporting such symptoms. Based on the results, the researchers warned:13
What Explains the Increased Risk of COVID-19?From their observations in the medical setting, the researchers arrived at the theory that PPIs may increase COVID-19. “We developed this hypothesis at the beginning of the COVID-19 pandemic when we started to see a high incidence of GI symptoms and learned that the virus sheds into saliva, and thus can be swallowed into the stomach," said Dr. Christopher V. Almario, the study's lead author.14 The basis of the findings is likely PPIs' induction of a condition called hypochlorhydria, a low level of stomach acid, say the researchers. Hypochlorhydria impairs the body’s ability to defend against ingested bacteria and viruses. In one study, once-daily PPI use "increased the odds for enteric infection by 33%." Since it is known that pH ≤3 impairs the infectivity of a virus similar to COVID-19 (SARS-CoV-1), though its effect on COVID-19 is not yet known, the researchers wrote:15
The Researchers Discuss the StudyUpon hearing the results of the study, some who are taking PPIs may want to abruptly stop. But Dr. Brennan Spiegel, one of the study authors, cautions against it.16
H2RAs, medications like Pepcid, Tagamet and Zantac, generally available over the counter, are not linked to contracting COVID-19 in the research. They are considered safer than PPIs and their use is suggested as a way to discontinue PPIs by tapering off treatment.17 However, one H2RA, Zantac, has a red flag of its own. In 2019, the FDA said tests revealed the presence of the carcinogen N-nitrosodimethylamine (NDMA) in Zantac, whose generic name is ranitidine. According to Harvard Health Publishing:18
In April 2020, the FDA requested manufacturers to withdraw all prescription and over-the-counter Zantac drugs from the market.19 PPIs Are Dangerous Regardless of COVID-19 LinksPPIs are designed to reduce acid in the stomach, yet hydrochloric acid, along with pepsin, is necessary to break down protein in your intestinal tract. That means a reduction in acid from the use of PPIs changes nutrient absorption and digestion for the worse. Without adequate breakdown of protein, you increase the risk of experiencing dysbiosis,20 or an imbalance in the gut microbiome between pathogenic bacteria and friendly bacteria. This condition opens the door for a host of other problems like candida, Helicobacter pylori (H. pylori), C. difficile and leaky gut. Moreover, when people suffer from heartburn, GERD and chronic indigestion, the problem is rarely caused by too much acid. Patients with these ailments are usually suffering from other stomach issues that can be addressed with a healthy diet and natural treatments. Unless an endoscopy has confirmed high levels of stomach acid, it's actually more likely that you don't have enough. PPIs Have Serious Side Effects and Limited UsesAccording to gastroenterologist Dr. Mitchell Katz, PPIs are warranted for only a few conditions, including:21
Prescribing PPIs for other conditions is irresponsible because they are linked to many concerning conditions, as I’ve noted. According to The New York Times:22
PPIs are especially problematic for seniors, wrote the Times. Dr. Ian Logan, a Scottish physician, said:23
Among the side effects often seen are increased risk of pneumonia, gastrointestinal infections and severe diarrhea. Here are more scientifically documented risks of PPIs:
How to Wean Off PPIsIf you’re already taking a PPI, you'll want to get on a lower dose than you're on now, if possible, and then gradually decrease your dose even further. Once you get down to the lowest dose of the PPI, you can start substituting with an over-the-counter H2 blocker like Tagamet or Cimetidine, but not Zantac or ranitidine. Then, gradually wean off the H2 blocker over the next several weeks while implementing the lifestyle strategies addressed below. As always, be sure to check with your doctor before starting any new medications or making changes to the ones you’re currently taking.
There Are Many Safe Alternatives to PPIsIn summary, PPIs are linked to many serious side effects for which the 7.8% of the U.S. adult population who take them may be at risk. Yet, the painful, acid-based conditions that people take PPIs for can often be relieved by making relatively simple lifestyle changes. These changes are especially important with the reported links between PPIs and COVID-19. from http://articles.mercola.com/sites/articles/archive/2020/07/22/antacids-can-increase-risk-of-covid.aspx A largely hidden issue of the COVID-19 pandemic is the risk of medical malpractice, and the consequences for patients, health care workers and hospitals alike. As noted by Epic Brokers:1
Indeed, New Jersey2 has granted full immunity — both civil and criminal — to health care providers battling COVID-19. Sweeping civil and criminal immunity has also been granted in New York. New York Governor Andrew Cuomo who, against federal guidelines, ordered ill equipped nursing homes to accept COVID-19 patients, also granted immunity to nursing home executives. The immunity rule was reportedly3 issued after the Greater New York Hospital Association donated more than $1 million to the New York State Democratic Committee. Two New York legislators have since introduced a bill that would repeal Cuomo’s blanket immunity.4 Michigan, Massachusetts, Illinois and Connecticut have also issued immunity laws,5 and Iowa lawmakers introduced a bill to grant broad protections to health care providers, hospitals, nursing homes and a variety of other businesses in early June.6 Medical Errors Are Third Leading Cause of Death in the USThe problem with handing out broad immunity to any and all health care providers and executives is that it may lower the quality of care. If you know you cannot be sued under any circumstance, you’re less likely to take all the precautions necessary to avoid making a mistake. It is likely this immunity to prosecution led to the egregious ethical and medical breeches documented by the undercover nurse Erin Marie Olszewski at the epicenter of the pandemic, Elmhurst Hospital in New York, which you can see in the section below. Even without the pandemic, medical errors are the third leading cause of death in the U.S., according to Johns Hopkins patient safety experts.7 According to their data, 9.5% of all annual deaths stem from medical errors, including misdiagnoses and treatment mistakes. The situation may be even worse than that, however. According to the 2017 paper,8 “Your Health Care May Kill You: Medical Errors,” more than 90% of medical errors go unreported. Even so, medical error rates in the U.S. are “significantly higher” than those in other developed countries, including Canada, Australia, New Zealand, Germany and the U.K., the paper notes.9 The 2017 Commonwealth Fund report,10 “Mirror, Mirror 2017: International Comparison Reflects Flaws and Opportunities for Better U.S. Health Care” also points out that the U.S. health care system continually ranks LAST in patient outcomes when compared to other high-income nations. This, despite the fact that the U.S. health care system outspends all other countries. Nurse on the Frontlines of COVID-19 Shares Her ExperienceWhile it’s important to not hold health care workers to irrational standards in the midst of an outbreak of a novel, never-before-seen disease, giving everyone a free pass no matter how obviously egregious their negligence can also put patients at unnecessary risk. A standout case in point is the Elmhurst Hospital Center, a public hospital in Queens, New York, which has been “the epicenter of the epicenter” of the COVID-19 pandemic in the U.S. In a heavily censored interview, nurse Erin Olszewski addresses a number of problems at Elmhurst, including the hospital’s:
Of these, the seemingly systematic mislabeling of negative COVID-19 tests as positive and the routine use of mechanical ventilation are perhaps the most abhorrent, as it has undoubtedly led to the unnecessary death of many. In her undercover video, Olszewski talks about how a stroke patient ended up contracting the disease due to being placed in the same room as a COVID-positive patient. He ended up on mechanical ventilation, drastically increasing his chances of dying due to lung damage. Part of why mechanical ventilation is so dangerous is because you are given sedatives and paralytics. You’re essentially asleep for the duration, which could be up to a month. “There’s no way you can recover from something like that,” Olszewski says. What’s worse, according to Olszewski, many patients are not even told that they will be put to sleep. They’re merely told they will receive breathing assistance. In a chilling conversation, a physician states that not a single patient has been successfully extubated and released since the pandemic began, and many of these weren’t even COVID-19 positive to begin with. In a case like this, should hospital staff and administrators really get off scot-free? July Is Medical Malpractice Awareness MonthA July 2, 2020, blog post11 by the law firm Ashcraft & Gerel lists “10 surprising facts about medical negligence and error in the U.S.” Among them:
Despite the continuous rise in preventable medical errors, the rate of successful medical malpractice claims declined 55.7% between 1992 and 2014. Even when there’s strong evidence of negligence, physicians are acquitted half of the time, and up to 90% of medical malpractice claims are dropped without payout. Pandemic Accelerates Risk Management ChangesAccording to The Health Care Blog,12 “the pandemic might ultimately … accelerate changes in the way health care organizations think about risk management and their insurance coverage for it.” In the video above, Margaret Nekic, CEO of Inspirien — a hospital-and-physician-owned medical malpractice and worker’s comp insurance company — discusses how liability carriers are responding to the changes brought by COVID-19. For example, during this pandemic, many doctors have been asked to provide care outside their area of expertise, which increases the risk of errors occurring. They’re also using modified equipment. Of course, SARS-CoV-2, being a novel virus, did not, and still doesn’t, have a clear-cut treatment strategy, and doctors have had to experiment and innovate. Health care workers are also providing testing outside of medical facilities, and while doctors are typically covered by their malpractice insurance regardless of where they work, most nurses are covered by the hospital in which they work, and may therefore not be covered if they’re providing testing or care in other facilities. The Problem With Standard of CareNow, while Johns Hopkins researchers have identified “unwarranted variation in physician practice patterns that lack accountability” as one of the primary contributors to medical errors,13 one could just as easily argue that the requirement to adhere to “standard of care” protocols may actually be part of the problem. Doctors are afraid to deviate from the standard of care, even when they disagree with it wholesale or believe it might not be in a specific patient’s best interest, because this is the easiest way to get sued for malpractice. It’s “easier” to let someone die than risk losing their medical license by doing something differently. This includes prescribing dangerous medications based on generalized recommendations rather than following a more individualized system of care. As it pertains to COVID-19, we’ve seen how Elmhurst hospital has continued using mechanical ventilation even though front-line workers and researchers have stepped forward, warning that ventilation kills more COVID-19 patients than it saves and doesn’t appear to be an appropriate treatment for this disease. We’ve also seen how early treatment with hydroxychloroquine and zinc, despite getting high marks from critical care doctors around the world, has been suppressed in the U.S. — based on fraudulent research, I might add — and both doctors and pharmacists have been warned they risk losing their medical license if they prescribe it.14 This, despite the fact that there really is no other carefully vetted COVID-19 treatment available yet, as potential therapeutics are still under investigation. ‘Pious’ Patients Are Most Likely to DieBack in 2012, I interviewed Dr. Andrew Saul about his book, “Hospitals and Health: Your Orthomolecular Guide to a Shorter Hospital Stay,” in which he discusses the risks hospitalized patients face. In it, he points out that knowing how to play “the hospital game” can help save your life. Importantly, so-called pious patients — those who keep quiet and question nothing — are the most likely to get killed. One of the best ways to safeguard your health and life during a hospital stay is to bring a personal advocate, someone who can speak up for you and ensure you’re given proper care — especially if you’re so sick you cannot do so yourself. Unfortunately, this pandemic has prevented family members from visiting those that are hospitalized to act as their advocates. Many times, this leaves them at the mercy of hospital staff and physicians that are immune from prosecution and negatively motivated to consider any natural therapy, even something as simple as vitamin D, for fear of repercussions from violating the “standard of care.” This makes it even more important, if you are ever hospitalized now, to question everything. It’s also important to remember you have the right to do so. As noted by Saul in that interview:
Surviving COVID-19There are no easy answers when it comes to COVID-19, but considering you may not have the ability to sue for malpractice under any circumstance (depending on where you live), taking a keen interest in your treatment would be advisable. I’ve written several articles over the past few months detailing some of the treatments that appear to be among the most effective, such as the MATH+ Protocol and early intervention with hydroxychloroquine and zinc. For home use, at first sign of symptoms, you could try quercetin in lieu of hydroxychloroquine, as the primary mechanism of action in COVID-19 is their ability to shuttle zinc into your cells, and it is the zinc that provides most of the benefits. Ketone esters may also be helpful for certain symptoms. Importantly, rather than waiting for a likely harmful vaccine, get proactive and start optimizing your vitamin D level. You can learn more about this in “The Most Important Paper Dr. Mercola Has Ever Written” and “How to Fix the COVID-19 Crisis in 30 Days.” As the old adage goes, an ounce of prevention is worth a pound of cure. Your safest bet to avoid becoming a medical error statistic is to stay out of the hospital, and to avoid hospitalization for COVID-19, you really need to focus on strengthening your immune function and reversing any underlying comorbidities such as insulin resistance and obesity. from http://articles.mercola.com/sites/articles/archive/2020/07/22/how-covid-19-affects-medical-malpractice.aspx As businesses and groups fluctuate between gathering or not, many have taken to doing a symptom check in the hope of reducing exposure to SARS-CoV-2. This usually consists of asking several questions, such as whether you have been exposed to anyone with an active infection or if you’ve had symptoms. The CDC recommended non-contact temperature assessments to be conducted at homeless shelters and encampments.1 Yet, the World Health Organization and the CDC acknowledge this may be inadequate since asymptomatic individuals might be able to spread the virus.2 Some companies in the U.S. instituted temperature checks for associates returning to work. Amazon announced they were doing this on more than 100,000 workers each day.3 Yet, in one study of 5,700 people triaged for hospitalization with COVID-19, researchers found only 30.7% had a fever.4 Infectious disease doctor from Johns Hopkins Center for Health Security, Dr. Amesh Adalja, spoke with a reporter from Health, saying:5
Data Show Smell and Taste Impairment Predicts COVIDThere has not been a definitive study on the number of people with COVID-19 who also have a fever.6 New research published in JAMA offers a clue that fever may not be as common with the virus as originally believed. Until more information is available, scientists are relying on data from the SARS epidemic in 2003 to assess COVID-19 patients. In one literature review published in 2009 following SARS, the researchers found that fever had a negative predictive value ranging from 86.1% to 99.7%.7 This means that those without a fever likely did not have SARS. However, the same cannot be said for COVID-19, as some people are contagious before they run a fever, and others may never get a fever. While temperature taking may only catch a small number of those with an infectious disease, some experts are suggesting that adding a smell test to screenings would be more effective. It's also important to remember that you can run a fever for reasons other than COVID-19. There is a growing body of evidence to suggest that people with the virus have a higher rate of smell and taste dysfunction, including complete loss, which is called anosmia (loss of sense of smell) and ageusia (taste). Andrew Badley is a leader of a virus lab at Mayo Clinic. He spoke with a Stat News reporter, saying:8
What Are the Numbers?Badley and his colleagues published a study in April in which they evaluated the clinical notes of 77,167 patients who had undergone PCR testing for COVID-19.9 They compared those results to the patients’ electronic health records and found that 2,317 were positive and 74,850 were negative. The team then identified and analyzed symptoms associated with COVID-19, including fever and chills, respiratory difficulty, cough, muscle pain, diarrhea and smell dysfunction. Those who tested positive were 27.1 times more likely to have smell and taste dysfunction than those who were negative. This was significantly higher than any other symptom analyzed. The closest was fever and chills, which presented a 2.6 times greater likelihood that the person would have the virus. In a separate study published in the International Forum of Allergy and Rhinology, researchers did a retrospective review of patients who came to the San Diego Hospital system between March 3, 2020 and April 8, 2020.10 They included those with a confirmed positive infection who also had an evaluation of smell and taste function. There were 128 who met the criteria. Of those, 20.1% required hospitalization. In further analysis, the team demonstrated:11
Data gathered from 220 survey respondents across the U.S. showed the symptom of loss of smell or taste was even higher.12 Of the respondents, 42% were COVID-19 positive and 58% were not. The loss or alteration in smell or taste as the first or sole symptom occurred in 37.7%. Separately, a review of the literature was conducted to include 24 studies from 8,438 lab-confirmed positive COVID-19 patients across 13 countries.13 The researchers found smell dysfunction was found in 41% and taste dysfunction was present in 38.2% of the population. Why Might Smell and Taste Be Affected?Dr. Justin Turner from Vanderbilt University Medical Center believes the prevalence of anosmia in the population with COVID-19 is 25%, and it may be as high as 80%, based on patients’ subjective reports.14 He also hypothesized how it may happen. He believes the primary cause is an inflammatory reaction brought about by the virus inside the nasal cavity near the olfactory nerve. He explains:15
Infection of the nasal epithelium also appears to be higher in adults. The authors of a study published in the Journal of the American Medical Association linked the low infection rate in children (less than 2%) with the hypothesis that they have a lower expression of ACE2 receptors than adults. They found that age was a risk factor based on the number of ACE2 receptors in the nasal cavity, “the first point of contact for SARS CoV-2 and the human body.”16 Your sense of taste is dependent on smell, so it makes sense that when smell is altered you also have an alteration in taste. I also wonder how much zinc deficiency or insufficiency may have to do with the loss of smell. Data gathered for a study published in the International Forum of Allergy and Rhinology showed that those who were admitted with more severe disease had an intact sense of taste and smell. One of the symptoms of zinc deficiency is a loss of sense of smell.17 We know the body uses zinc intracellularly to stop viral replication and slow or stop the infection.18 Could it be that individuals who get more zinc into the cells and use it to slow the infection also demonstrate symptoms of zinc insufficiency or deficiency as their body uses the trace element to fight the virus? How to Test for Zinc DeficiencyZinc is important to all organs and cell types, which explains the varied symptoms associated with deficiency. It is required for approximately 100 enzymes and is crucial for your immune function, wound healing, cell division and growth and development. Researchers believe that zinc deficiency:19
In North America, overt deficiency is uncommon and related to inadequate intake, increased losses or requirements. For instance, bioavailability is lower with a plant-based diet and some have found that vegetarians need 50% more of the recommended daily allowance than those who eat meat. However, it is not uncommon to have a mild or moderate zinc insufficiency. Since the trace element is important in the fight against viruses, including SARS-CoV-2, you may want to consider taking a simple zinc test at home to determine your status. In the video below Dr. Donald Ozello demonstrates a simple taste test that can quickly tell you how insufficient or deficient in zinc you might be. Simply place two tablespoons of a solution of zinc at room temperature in your mouth and hold it. The results are based on what you taste after 10 seconds.
Combine Quercetin and Zinc for a Powerful Immune BoostFor zinc to work it must first get into the cell. Your body uses zinc ionophores, or substances that open the cell membrane for it to pass through. Drugs like chloroquine and hydroxychloroquine are zinc ionophores, which likely explains how they affect those with COVID-19 when the drugs are combined with zinc. The good news is there are other substances that have the same action without the side effects. In a lab study published in 2014, scientists evaluated quercetin and epigallocatechin gallate (EGCG found in green tea) for the biological activity that may increase cellular zinc uptake. They concluded:20
Quercetin and EGCG also have the advantage of inhibiting an enzyme used by coronavirus to infect healthy cells.21 Adding to this, quercetin has potent antiviral activity in its own right.22 When considering supplementation, it's important to remember that excessive zinc may increase health risks. Acute side effects include nausea, vomiting, diarrhea, abdominal cramps and headaches.23 Another important factor relating to immune health is the balance of copper and zinc; an increased intake of zinc may help. Chris Masterjohn writes this as little as 60 milligrams of zinc per day can introduce problems.24 Essentially, copper lowers the activity of superoxide dismutase, sometimes called SOD. This is a crucial to your immune defense. He recommends:
from http://articles.mercola.com/sites/articles/archive/2020/07/22/can-smell-test-be-more-accurate-than-fever-for-covid.aspx In an effort to combat “misinformation,” the United Nations has enlisted 10,000 “digital volunteers” to rid the Internet of so-called “false” information that’s supposedly worsening the COVID-19 pandemic. As news outlet Devex reported, Melissa Fleming, the U.N.’s under-secretary-general of global communications, said, “Good information is how we’re going to overcome the virus,” adding:1
While it sounds altruistic to volunteer your time to combat the spread of misinformation, what the campaign, dubbed the Verified initiative, amounts to is an army of trolls engaging in censorship in an attempt to shut down opposition or opinions that run counter to the status quo. Trolls Enlisted to Combat ‘Communication Crisis’Upset by the fact that individuals are using social media and their immediate social circles to share information they deem relevant about COVID-19, the U.N. is asking the public to sign up to become “information volunteers” who commit to sharing “U.N.-verified, science-based content to keep their families and communities safe and connected.”2 If you sign up, you’ll get a daily briefing full of information the U.N. wants you to share, centering on three themes:3 1. Science — to save lives 2. Solidarity — to promote local and global cooperation 3. Solutions — to advocate support for impacted populations The information will come in easy-to-share formats optimized for social media in order to directly counter misinformation or fill an information void. Their primary audience is a vague “those who are being targeted with misinformation,” Fleming said,4 calling COVID-19 not just the century’s largest public health emergency, “but also a communication crisis.” She warns:5
The major red flag to the U.N.’s campaign is a lack of detail about what constitutes a “conspiracy theory” or “cure with no evidence to back it up.” Some of the information Verified is aiming to share simply states, “If you come across a post online that makes you really angry or frightened, it’s a sign you might be looking at misinformation.”6 Other suggested shares — found on the Verified U.N. site in posterboards with social media widgets on them, state, “Misinformation spreads faster when we’re upset,” and shares information that downplays the importance of vaccine choice and open conversation regarding their safety, especially as a COVID-19 vaccine is being fast-tracked to the market: “Vaccines are safe and they help prevent millions of deaths every year. Yet, a growing number of networks seek to undermine trust in vaccinations.”7 UN Calls for Global Fight Against ‘Infodemic’In a statement released by the Republic of Latvia’s Ministry of Foreign Affairs, countries are called on to step up and support the U.N.’s mission to counter the “infodemic” that they claim is “as dangerous to human health and security as the pandemic itself:”8
Ironically, in outlining the “crucial need for access to free, reliable, trustworthy, factual, multilingual, targeted, accurate, clear and science-based information,” they call on countries to take steps to stop the spread of information they deem to be false and to spread information from “trustworthy sources,” which is the U.N.’s Verified campaign. One-hundred thirty-two member states, non-member observer states and observers have so far endorsed their statement, which reads in part:
Is the UN’s New World Order Advancing?Many aren’t aware that on March 19, 2020, the United Nations New World Order (UNNWO) launched its annual campaign to celebrate an international happiness day, which its website says it has celebrated every year since 2012.9 If you haven’t heard of UNNWO, its website starts out with, “Let’s take our planet back,” On March 19, it then read:10
That note was taken down, though, sometime afterward, with no records of it in Wayback internet archives showing up until May 3, 2020,11 and by that time the page had been changed to buttons on the movement’s initatives and goals. Today the website has no clickable buttons and reads only “Let’s take our planet back.”12 Its initiatives, still listed in the Wayback archives, include “happytalism,” which “places happiness, well-being, and freedom at the center of human development models, systems, and all life.” It also supports the mobilization of more than $30 trillion toward achieving the 17 UN Global Goals by 2030, which include things like no poverty, zero hunger, gender equality and clean water and sanitation. It sounds like utopia, but some believe the push for a one-world government isn’t about pushing forward world peace and happiness but, rather, about taking rights away from the public and putting the power into the hands of a select few.13 Censorship of media and social media is already filtering information and telling people what they should and shouldn’t fear, and increased surveillance is being pushed courtesy of coronavirus. The U.N.’s Verified initiative fits in nicely with this plan and is being orchestrated in collaboration with Purpose, a social mobilization organization. According to Fleming, even social media platform’s highly suspect acts of taking down “dubious information” or directing users to government health websites isn’t enough to protect the public. “But this is not enough,” she says, “particularly because the most pernicious misinformation and conspiracy content spreads via messaging apps, peer-to-peer.”14 The World Health Organization also has an Immunization Agenda 2030, in which they’re aiming to vaccinate everyone across the globe: “IA 2030 envisions a world where everyone, everywhere, at every age, fully benefits from vaccines to improve health and well-being.”15 The Bill & Melinda Gates Foundation is the biggest funder of WHO, and Bill Gates intends to vaccinate the global population against COVID-19, and then track and monitor each one through digital surveillance. Some of the U.N.’s Verified content likewise states, “As experts work around the clock to develop a vaccine for COVID-19 we must all play our part to ensure it is ‘a people’s vaccine’ — available to all.” And they quote vaccine advocate Ethan Lindenberger, who says, “If I get immunized, I’m contributing to the personal health and safety of everyone around me.”16 There’s no reason in the world to believe this gigantic global disease surveillance system would be dismantled once the pandemic is declared over. Naturally, it will simply transition into other surveillance functions. More Internet Censoring ToolsThe U.N.’s verified campaign is reminiscent of another self-appointed internet watchdog, NewsGuard, which claims to rate information as “reliable” or “fake” news, supplying you with a color-coded rating system next to Google and Bing searches, as well as on articles displayed on social media. If you rely on NewsGuard’s ratings, you may decide to entirely skip by those with a low “red” rating in favor of the “more trustworthy” green-rated articles — and therein lies the problem. NewsGuard is in itself fraught with conflict of interest, as it’s largely funded by Publicis, a global communications giant that’s partnered with Big Pharma, such that it may be viewed more as a censorship tool than an internet watchdog. For example, NewsGuard announced that my site has been classified as fake news because we have reported the SARS-CoV-2 virus as potentially having been leaked from the biosafety level 4 (BSL4) laboratory in Wuhan City, China, the epicenter of the COVID-19 outbreak. According to NewsGuard, “There is no evidence that the Wuhan Institute of Virology was the source of the outbreak, and genomic evidence has found that the virus is 96% identical at the whole-genome level to a bat coronavirus.”17 But NewsGuard’s position is in direct conflict with published scientific evidence suggesting this virus was created in a lab and not zoonotically transmitted. Thus, by giving a falsely low rating and “censoring” my site, they’re doing a disservice to people looking for trustworthy information and in and of themselves are spreading misinformation. By enlisting an army of trolls to spread their own rhetoric, the concern is that the U.N.’s Verified campaign will do more of the same. Share the Information You Believe InUltimately, most adults are fully capable of choosing what information they deem credible to share with their social networks, family and friends, without the need for an overreaching Big Brother telling them what’s credible and what’s not. What is important is always looking at the source of the information and the motives behind it, something even the U.N.’s Verified touts. Toward this end, the U.N. is closely partnered with the World Health Organization. Only 25% of WHO’s funding comes from member states. The remaining 75% comes from voluntary contributions. The Bill & Melinda Gates Foundation — the investments of which include junk food manufacturers, alcohol and drug retailers — is the biggest funder.18 from http://articles.mercola.com/sites/articles/archive/2020/07/21/un-unleashes-army-of-trolls-to-shut-down-opposition.aspx In July 2020, famous Broadway actor Nick Cordero died of complications from COVID-19, including septic shock, or sepsis.1 Sepsis is a life-threatening condition triggered by a systemic infection that causes your body to overreact and launch an excessive and highly damaging immune response. Unless promptly diagnosed and treated, it can rapidly progress to multiple-organ failure and death. Sepsis is common, affecting at least 1.7 million Americans every year and leading to 270,000 deaths. In hospitals, 1 in 3 patients who die have sepsis, according to the U.S. Centers for Disease Control and Prevention,2 and it’s a major contributing factor to influenza deaths.3 Not only is sepsis a leading cause of deaths overall, it’s also an important contributor to the death of COVID-19 patients — one that’s been flying largely under the radar. Many Critically Ill COVID Patients Develop SepsisResearchers from China wrote in The Lancet, “In clinical practice, we noticed that many severe or critically ill COVID-19 patients developed typical clinical manifestations of shock, including cold extremities and weak peripheral pulses, even in the absence of overt hypotension. Understanding the mechanism of viral sepsis in COVID-19 is warranted for exploring better clinical care for these patients.”4 Viral sepsis can be particularly challenging, according to the Sepsis Alliance, because tests that reveal bacterial sepsis to physicians do not necessarily reveal viral sepsis. That being said, abnormal vital signs, including blood pressure, pulse and respirations, may occur with either bacterial or viral sepsis. Dr. Karin Molander, chair of the Sepsis Alliance board of directors, explained, “Studies coming out of Wuhan, China, and our experts here in the U.S. are finding that sepsis is a leading, if not the number one, fatal complication of COVID-19.”5 Sepsis occurs so often alongside COVID-19 that the National Center for Health Statistics released updated guidelines for medical coding of the two conditions.6 In a Q&A by the Association of Clinical Documentation Integrity Specialists (ACDIS) Leadership Exchange, a commentator asked, “I’m not clear if we still follow sequencing direction included in the Official Guidelines for Coding and Reporting which states that we should code first for sepsis followed by infection. This would make more sense to me …”7 In response, ACDIS noted, “When COVID-19 meets the definition of principal diagnosis, code U07.1, COVID-19, should be sequenced first, followed by the appropriate codes for associated manifestations …” The updated guidelines suggest that whether or not coding for COVID-19 or sepsis occurs first depends on their sequencing (if the patient has sepsis upon hospital admission or developed it after admission, for instance).8 Who’s at Risk of Sepsis?According to Sepsis Alliance, “the elderly, very young and people with chronic illnesses or weakened immune systems” are most at risk of sepsis.9 Because people requiring home health care are at increased risk for COVID-19 and other infections, as well as sepsis, the Sepsis Alliance partnered with Elara Caring, a U.S. provider of home-based health care, to improve care and outcomes for COVID-19 patients with sepsis in the home care setting.10 Staff will receive increased education and training on sepsis prevention and care, which could be life-saving, since early detection and treatment can mean the difference between life and death in sepsis cases, which often start in the community from an infection caused by bacteria or a virus, parasite or fungus. The immune response triggered by an infection may lead to leaky blood vessels, blood clots, poor blood flow and, in severe cases, organ failure.11 When blood pressure drops in combination with a weakened heart it leads to septic shock. As mentioned, the underlying trigger, an infection, often starts in the community. This may explain why it is often misdiagnosed in the beginning, which increases the potential risk for disability and death. While those affected often have underlying health conditions, even healthy people can be affected. “[W]hen a healthy person becomes severely ill with sepsis, it could be that their healthy immune system was so strong it triggered a cytokine storm,” the Sepsis Alliance explained.12 The Cytokine Storm ConnectionCytokines are a group of proteins that your body uses to control inflammation. If you have an infection, your body will release cytokines to help combat inflammation, but sometimes it releases more than it should. If the cytokine release spirals out of control, the resulting “cytokine storm” becomes dangerous and is closely tied to sepsis. Dr. Molander said:13
The symptoms of cytokine storm are indicative of severe illness and include high fever, severe fatigue, nausea and organ failure. “Most of these severely ill patients receive treatment in an ICU or high acuity unit. There they may receive experimental medications like interleukin antibodies, such as anti-IL-1 or anti-IL-6 and high dose corticosteroids to try to get the cytokine storm under control,” according to the Sepsis Alliance.14 Natural options have also shown promise for alleviating cytokine storms, including:
Vitamin C Shows Promise for COVID-19, SepsisIn my March 17, 2020, interview with Dr. Andrew Saul, editor-in-chief of the Orthomolecular Medicine News Service, Saul mentions being in contact with a South Korean medical doctor who is giving patients and medical staff an injection of 100,000 IUs of vitamin D along with as much as 24,000 mg (24 grams) of IV vitamin C. "He's reporting that these people are getting well in a matter of days," Saul says. As explained by Saul, vitamin C at extremely high doses acts as an antiviral drug, actually killing viruses. While it does have anti-inflammatory activity, which helps prevent the massive cytokine cascade associated with severe SARS-CoV-2 infection, its antiviral capacity likely has more to do with it being a non-rate-limited free radical scavenger. Rhonda Patrick, Ph.D. also noted that vitamin C may be protective against respiratory diseases. In one study, people with the highest vitamin C levels were 15% less likely to develop respiratory conditions and 46% less likely to die of lung cancer compared to those with the lowest levels.19 Further, vitamin C is well known for helping with lung defense, which takes on renewed meaning in the midst of the COVID-19 pandemic. According to Patrick:20
Of note, vitamin C is also useful for sepsis. A 2019 study using vitamin C found it lowered mortality risk in patients with severe sepsis, and reduced the number of days spent in intensive care and overall hospital stay.21 Dr. Marik’s Vitamin C ProtocolA sepsis treatment protocol developed by Dr. Paul Marik, a critical care doctor at Sentara Norfolk General Hospital in East Virginia, which involves intravenous (IV) vitamin C with hydrocortisone and thiamine (vitamin B1), has been shown to dramatically improve chances of survival in sepsis cases.22 His retrospective before-after clinical study showed that giving patients 200 milligrams (mg) of thiamine every 12 hours, 1,500 mg of ascorbic acid every six hours, and 50 mg of hydrocortisone every six hours for two days reduced mortality from 40% to 8.5%.23 “Our results suggest that the early use of intravenous vitamin C, together with corticosteroids and thiamine, are effective in preventing progressive organ dysfunction, including acute kidney injury, and in reducing the mortality of patients with severe sepsis and septic shock,” Marik and colleagues wrote in the journal Chest.24 Research published in 2020 found Marik’s sepsis vitamin C protocol lowered mortality in pediatric patients as well.25 As noted by the authors, “Our results suggest that HAT [hydrocortisone, ascorbic acid and thiamine] therapy, when administered early in the clinical course, reduces mortality in children with septic shock.” While each part of the protocol is safe on an individual basis, the three parts must be administered together to work effectively. Marik explained the combination targets multiple areas of the body's response to an infection and helps restore the dysregulated immune response.26 This then helps prevent organ failure and death. He goes on to discuss the excess production of reactive oxygen species underlies many of the damaging processes in sepsis. His team found the optimal dose of vitamin C was about 6 grams per day. Common Signs of SepsisThe symptoms of sepsis may be confused with those of a bad cold or flu, and include:27
Sepsis is a medical emergency, so if you suspect you may have it, get medical help immediately. Marik's sepsis protocol can be a lifesaver, so you'd be wise to discuss it with your doctor any time you're hospitalized. This way, should you develop sepsis while you're admitted, your medical team already knows your wishes and can act swiftly. According to Marik, the best results are obtained when the protocol is administered within the first six hours of presentation of symptoms.28 from http://articles.mercola.com/sites/articles/archive/2020/07/21/why-are-so-many-covid-patients-dying-of-sepsis.aspx According to a British observational study1 posted July 6, 2020, on the preprint server medRxiv, ultraviolet (UV) radiation exposure appears to lower COVID-19 mortality rates. As reported by News Medical Life Sciences,2 environmental factors such as temperature, humidity and UV irradiation are known to play a role in other infectious diseases, including seasonal influenza, so it shouldn’t come as a surprise that SARS-CoV-2 — the virus responsible for COVID-19 — can be affected in a similar manner. UV Radiation Lowers COVID-19 MortalityI’ve written extensively about the importance of vitamin D and its influence on COVID-19 specifically, but this research suggests there are other benefits to sun exposure besides vitamin D production. The researchers looked at UVA measures and COVID-19 death statistics in 2,474 U.S. counties, 6,755 Italian municipalities and 6,274 areas in England between the months of January and April 2020, which is when vitamin D production due to low sun exposure tend to be minimal. According to the authors:3
Mechanisms of ActionThe researchers hypothesize UV exposure “may have a direct effect on the viability of SARS-CoV-2 virus in airborne droplets,” as well as the virus’ ability to stay viable on various surfaces, thus reducing overall infection rates and lowering the initial inoculation load in those infected, which in turn might reduce the risk of severe illness. Another mechanism of action may involve nitric oxide. UVA radiation triggers the release of nitric oxide in your skin, mobilizing it into your circulation. This lowers blood pressure by causing your blood vessels to expand. This, the researchers say, is one important metabolic benefit of UV exposure that does not involve vitamin D.
What’s more, nitric oxide may help mitigate the endothelial damage seen in severe COVID-19 infection that leads to organ failure. While not mentioned in this study, nitric oxide also improves your immune function, thins your blood and decreases blood viscosity, which in turn decreases platelet aggregation. As such, nitric oxide helps reduce your risk of developing a life-threatening blood clot. Previous research has also found nitric oxide inhibits replication of the SARS virus (SARS-CoV), and the researchers hypothesize that, since the spike proteins of the two viruses are similar, nitric oxide may have a similar effect on SARS-CoV-2. If correct, this could be yet another mechanism of action by which nitric oxide helps reduce disease transmission and severity. So, to summarize, not only does exposure to sunlight lower COVID-19 mortality, but just about any strategy that boosts nitric oxide production may also have a similar effect. Examples of such strategies include the Nitric Oxide Dump workout and consuming nitrate-rich foods such as beetroot juice, arugula and cilantro. Are Stay-At-Home Orders Increasing COVID-19 Mortality?In related news, another study4 posted on medRxiv, July 2, 2020, asks whether lockdown orders might do more harm than good by decreasing the protective role of UVB radiation — the kind that triggers vitamin D production in your skin — which has also been shown to lower COVID-19 mortality rates. As noted by the authors:
According to their calculations, mortality rates could have been reduced by an average of 21% had lockdown orders been accompanied by instructions to get regular sun exposure. Vitamin D Lowers All COVID-19 Related RisksAs reviewed in several previous articles, vitamin D appears to impact virtually all COVID-19 related risks, including your risk of testing positive for active infection, disease severity and your risk of death. For example:
Higher Vitamin D Lowers All-Cause Mortality RiskCOVID-19 certainly isn’t the only disease influenced by vitamin D. As noted in a study14 published July 4, 2020, in the Journal of Clinical Endocrinology and Metabolism, higher vitamin D levels are “non-linearly linked to lower risk of all-cause, [cardiovascular disease] CVD, and cancer mortality.” Interestingly enough, this study found the risk for CVD and all-cause deaths tapered off at a vitamin D level of just 24 ng/mL (60 nmol/L). Cancer deaths leveled off at a mere18 ng/mL (45 nmol/L). This is surprisingly low, considering large-scale studies suggest the cutoff for optimal cancer protection is around 40 ng/mL (100 nmol/L), with a level of 60 ng/mL to 80 ng/mL (150 nmol/L to 200 nmol/L) being ideal for health and disease prevention. You can learn more about this in “For Optimal Health, Make Sure You Have a Vitamin D Level of 60 ng/mL.” Magnesium Optimizes Vitamin D SupplementationAccording to a scientific review15,16 published in 2018, as many as 50% of Americans taking vitamin D supplements may not get significant benefit as the vitamin D simply gets stored in its inactive form, and the reason for this is because they have insufficient magnesium levels, and magnesium is required in the conversion of vitamin D into its active form. Research17 published in 2013 also highlighted this issue, concluding that higher magnesium intake helps reduce your risk of vitamin D deficiency by activating more of it. More recently, research18 by GrassrootsHealth reveals you need 146% more vitamin D to achieve a blood level of 40 ng/ml (100 nmol/L) if you do not take supplemental magnesium, compared to taking your vitamin D with at least 400 mg of magnesium per day. 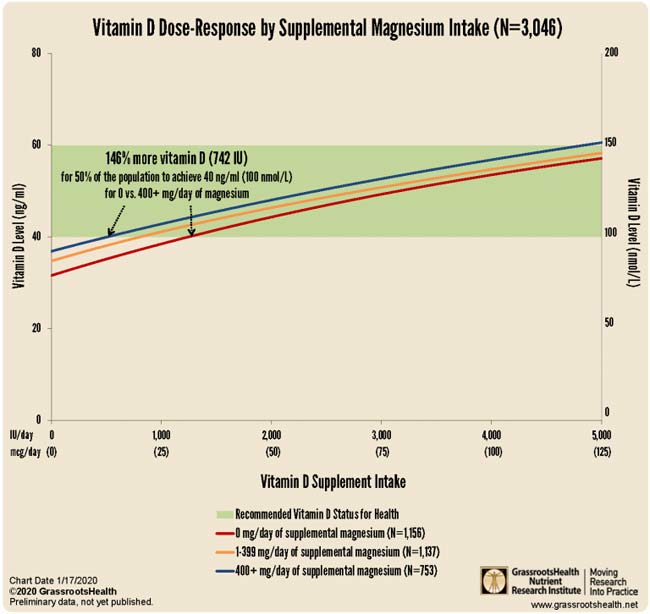
You can cut your need for oral vitamin D even further — by as much as 244% — by taking it concurrently with both magnesium and vitamin K2, as reported in “Magnesium and K2 Optimize Your Vitamin D Supplementation.” Optimize Your Vitamin D Level to Minimize COVID-19 RisksWhile oral vitamin D supplementation may be a good idea for most people, it’s important to remember to get your vitamin D level tested first. The reason for this is because you cannot rely on blanket dosing recommendations. The crucial factor here is your blood level, not the dose, as the dose you need is dependent on several individual factors, including your baseline blood level. I recently published two vitamin D reports, a comprehensive scientific review and a shorter summary, in which I detail vitamin D’s mechanisms of action and how to ensure optimal levels. I recommend downloading and sharing those reports with everyone you know. 
Here’s a condensed summary of the key steps to optimizing your vitamin D: 1. First, measure your vitamin D level -- One of the easiest and most cost-effective ways of measuring your vitamin D level is to participate in the GrassrootsHealth’s personalized nutrition project, which includes a vitamin D testing kit. You also have the option of testing vitamin D in conjunction with magnesium and omega-3. Once you know what your blood level is, you can assess the dose needed to maintain or improve your level. If you cannot get enough vitamin D from the sun (you can use the DMinder app19 to see how much vitamin D your body can make depending on your location and other individual factors), then you’ll need an oral supplement. 2. Assess your individualized vitamin D dosage -- To do that, you can either use the chart below, or use GrassrootsHealth’s Vitamin D*calculator. To convert ng/mL into the European measurement (nmol/L), simply multiply the ng/mL measurement by 2.5. To calculate how much vitamin D you may be getting from regular sun exposure in addition to your supplemental intake, use the DMinder app.20 Remember, you won’t need as much oral vitamin D if you also take magnesium and vitamin K2, as discussed above. 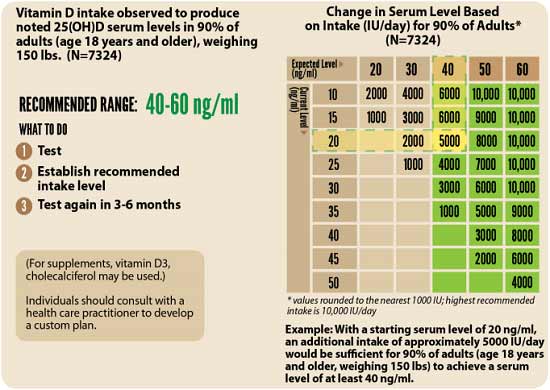
3. Retest in three to six months -- Lastly, you’ll need to remeasure your vitamin D level in three to six months, to evaluate how your sun exposure and/or supplement dose is working for you. from http://articles.mercola.com/sites/articles/archive/2020/07/21/coronavirus-uv-radiation.aspx |
Nia Pure NatureThe Provider of premium Quality Health Products To Live Better Lives Archives
March 2022
Categories |
 RSS Feed
RSS Feed
