|
This Mercury-Free Dentistry Week, we celebrate the 20th anniversary of Consumers for Dental Choice, the nonprofit advocates moving mercury-free dentistry from dream to reality. From protecting dentists' right to practice without mercury-laden dental amalgam fillings to obtaining mandated fact sheets to inform patients about amalgam's mercury content, to bans and restrictions on amalgam use around the world, Consumers for Dental Choice and its leader, former state Attorney General Charlie Brown, are making mercury-free dentistry more widely available than ever before. And, that progress is starting to sway the U.S. Food and Drug Administration (FDA), the chief regulator of dental amalgam, at the federal level. Thanks to your donations, Consumers for Dental Choice has reopened the door for FDA action against amalgam. I ask that you continue your support by donating at ToxicTeeth.org, and I will match all donations during Mercury-Free Dentistry Week (August 23 to 29, 2020) up to $150,000. So, double your impact today. Together, we can win the campaign for mercury-free dentistry at FDA that has come so far. 
Consumers for Dental Choice Sues the FDA — and WinsThe FDA is legally required to classify — that is, issue a rule for — all medical devices, including dental amalgam. But for 30 years, FDA dodged its legal duty to classify amalgam. Consumers for Dental Choice put an end to FDA's negligence. In 2008, this dynamic nonprofit organization assembled plaintiffs and sued FDA, demanding that amalgam be classified. The judge agreed and told FDA to sit down with Consumers for Dental Choice to determine a deadline. FDA was compelled to commit to classifying amalgam by July 2009. But when July 2009 came around it was clear the FDA had not considered the science — especially the evidence of harm amalgam can cause vulnerable populations like children, pregnant women and breastfeeding mothers. Its abysmal rule reflected it, posing no restrictions on amalgam use to protect the public — or even requiring that patients be told that amalgam is made of mercury. Nonetheless, FDA's rule acknowledged that amalgam could be harmful and that there was no proof of safety for the populations most susceptible to this toxin:
Fortunately, Consumers for Dental Choice never puts all its eggs in one basket. So, Charlie and his team challenged FDA's rule while pursuing other opportunities to advance mercury-free dentistry, like defeating pro-mercury state dental boards, fighting for amalgam fact sheet laws for patients at the state level and getting amalgam into the Minamata Convention on Mercury. And as Consumers for Dental Choice racked up win after win — regaining licenses for mercury-free dentists persecuted by state boards, gaining fact sheets to protect dental patients, achieving an amalgam reduction requirement in the Minamata Convention — the FDA's rule became more and more outdated and the U.S. slipped further and further behind. Consumers for Dental Choice's Game-Changing Return to FDAAlmost a decade after the FDA issued its flawed amalgam rule, Consumers for Dental Choice launched a nonstop campaign focused on getting FDA moving again on amalgam. And that campaign is starting to bear fruit. To succeed, Consumers for Dental Choice brought a whole new ball game to the FDA, giving the agency even more reasons to act. First, Consumers for Dental Choice assembled an accomplished team of experts to approach the FDA. In 2018, they unveiled the Chicago Declaration to End Mercury Use in the Dental Industry at the University of Illinois School of Public Health. This declaration, signed by 50-plus heavy-hitter environmental groups, called on the FDA "to bring its policies in line with the Federal Government as a whole and with its responsibilities under the Minamata Convention and to publicly advise a phase down of the use of mercury amalgams with the goal of phasing out entirely." Furthermore, it recommended immediately ceasing amalgam use in children, pregnant women and breastfeeding mothers. Working with some key signatories to the Chicago Declaration, Consumers for Dental Choice sent the declaration to FDA — and their team got meetings with the top of the agency. Second, Consumers for Dental Choice organized a strong showing of public support from you. Do you remember its online petition that almost 50,000 of you signed? Consumers for Dental Choice presented it to the FDA in person at its first meeting with the agency and has continued to make sure your voice is heard via such means as the public comments on patient preferences it asked you to submit to the FDA last spring. As one article's headline described the result, "FDA Gets Mouthful on Mercury Dental Fillings After Requesting Public Comment on Device Regulation."1 Third, Consumers for Dental Choice presented the FDA with new science showing amalgam's harmful effects. FDA Flips Their Position on AmalgamHaving reached the top of the agency, Consumers for Dental Choice could submit scientific studies that someone at the FDA would read. As a result, FDA's most recent scientific review of amalgam flips FDA's position on a major issue. FDA now recognizes evidence that shows once dental amalgam is implanted in the human body, its elemental mercury can convert to toxic methylmercury — the same type of mercury that the FDA warns about in fish. Furthermore, FDA is starting to recognize the bioaccumulative effect of amalgam's mercury. With patients exposed to so many sources of mercury — from high-mercury fish in their diets, occupational exposures in their workplaces and waste incinerators emitting mercury in their neighborhoods — the mercury from amalgam could very well be the straw that breaks the camel's back. Consumers for Dental Choice laid a track record of victories on the table at the FDA. Working with strong local partners, Consumers for Dental Choice has won amalgam phase-out set dates in the Philippines, Ireland, Slovakia, Finland, Nepal, Moldova, Czech Republic and New Caledonia. Consumers for Dental Choice has also won — again partnering with a local partner — bans on amalgam use in children in the European Union, Vietnam and Tanzania, and public warnings about amalgam's mercury in Nigeria. And, it let the FDA know about these victories because if other countries can do it, so can the U.S. Armed with this new support, Consumers for Dental Choice succeeded in persuading the FDA to reopen the amalgam issue, starting with a new FDA review and scientific advisory committee meeting. Consumers for Dental Choice Convinces the FDAIn November 2019, the promised FDA scientific advisory committee met to discuss metal implants and specifically dental amalgam. First, the committee heard from the public, primarily Consumers for Dental Choice's team of 16 experts. Consumers for Dental Choice executive director Charlie Brown testified alongside 15 heavy hitters from the Children's Environmental Health Network, Tuskegee University, International Indian Treaty Council, Organic & Natural Health Association and Connecticut Coalition for Environmental Justice, as well as city and county commissioners, a physician expert in environmental justice, a pharmacist specializing in toxicology and several attorneys — all speaking out for mercury-free dentistry. You can see Consumers for Dental Choice's team and their colleagues in action in the video at the top of this article, which shares highlights of the advisory panel meeting. The FDA advisory committee members discussed amalgam among themselves. They recommended that the agency provide information to patients about the risks of dental amalgam, especially for vulnerable populations. Committee members expressed particular concern about the disproportionate use of amalgam in disadvantaged populations, including communities of color and low-income communities that are already exposed to higher levels of toxins. And many committee members even called for an end to amalgam use:
Even the FDA advisory committee chair, Dr. Rao, agreed as he summed up the committee's conclusions to the FDA:
So, the consensus of its own advisory committee is that FDA's silence on amalgam must end. But as executive director Charlie Brown explains:
Now It's Your Turn to ActConsumers for Dental Choice has brought a whole new ball game to FDA, and this time it looks like the FDA is ready to play ball. But you don't have to wait on the government; you can go to a mercury-free dentist now by checking out Consumers for Dental Choice's listing of mercury-free dentists. With your continuing support, this effective advocacy organization can make the dream of mercury-free dentistry a reality at the FDA. Will you consider a donation to this 501(c)(3) nonprofit organization dedicated to advocating mercury-free dentistry? If you donate during Mercury Awareness Week (August 23 to 29, 2020), I will double your money. I'll match you, dollar for dollar (up to $150,000). Donations are tax-deductible and can be made online at ToxicTeeth.org. Checks can be mailed to: Consumers for Dental Choice Thank you for helping make the dream of mercury-free dentistry into reality for all patients, everywhere.
from http://articles.mercola.com/sites/articles/archive/2020/08/27/mercury-use-in-dentistry-is-on-its-way-out.aspx
0 Comments
The lecturer in the featured video, Maryanne Demasi, Ph.D., produced the 2014 Australian Catalyst documentary, "Heart of the Matter: Dietary Villains," which exposed the cholesterol/saturated fat myths behind the statin fad and the financial links which lurk underneath. The documentary was so thorough that vested interests actually convinced ABC TV to rescind the two-part series.1 The Australian Heart Foundation, the three largest statin makers (Pfizer, AstraZeneca and Merck Sharp & Dohme) and Medicines Australia, Australia's drug lobby group, complained2 and got the documentary expunged from ABC TV. Cholesterol and saturated fat have been the villains of heart disease for the past four decades, despite the many studies showing neither has an adverse effect on heart health. The entire food industry shifted away from saturated fat and cholesterol, ostensibly to improve public health, and the medical industry has massively promoted the use of cholesterol-lowering statin drugs for the same reason. Despite all of that, the rate of heart disease deaths continues to be high.3 That really should tell us something. Statins Are a Colossal Waste of MoneySince the release of Demasi's documentary, the evidence against the cholesterol theory and statins has only grown. As noted in an August 4, 2020, op-ed by Dr. Malcolm Kendrick, a general practitioner with the British National Health Service:4
According to a scientific review5 published online August 4, 2020, in BMJ Evidence-Based Medicine, lowering LDL is not going to lower your risk of heart disease and stroke. "Decades of research has failed to show any consistent benefit for this approach," the authors note. Since the commercialization of statin drugs in the late '80s (lovastatin being the first one, gaining approval in 19876), total sales have reached nearly $1 trillion.7,8 Lipitor — which is just one of several brand name statin drugs — was named the most profitable drug in the history of medicine.9,10 Yet these drugs have done nothing to derail the rising trend of heart disease. Lowering Cholesterol Does Not Show a Beneficial ImpactAccording to a press release announcing the BMJ Evidence-Based Medicine review, the analysis found that:11
In their paper,12 the study authors argue that since dozens of randomized controlled trials looking at LDL-cholesterol reduction "have failed to demonstrate a consistent benefit, we should question the validity of this theory." They also cite the Minnesota Coronary Experiment,13 a double-blind randomized controlled trial involving 9,423 subjects that sought to determine whether replacing saturated fat with omega-6 rich vegetable oil (corn oil and margarine) would reduce the death rate from heart disease by lowering cholesterol. It didn't. Mortality and cardiovascular events increased even though total cholesterol was lowered by 13.8%. For each 30 mg/dL reduction in serum cholesterol, the death risk rose by 22%. In conclusion, the Evidence-Based Medicine study authors note that:14
Deception Through StatisticsIf lowering cholesterol doesn't reduce mortality or cardiovascular events, there's little reason to use them, considering they come with a long list of adverse side effects. Sure, there are studies claiming to show benefit, but many involve misleading plays on statistics. One common statistic used to promote statins is that they lower your risk of heart attack by about 36%.15 This statistic is derived from a 2008 study16 in the European Heart Journal. One of the authors on this study is Rory Collins, who heads up the CTT Collaboration (Cholesterol Treatment Trialists' Collaboration), a group of doctors and scientists who analyze study data17 and report their findings to regulators and policymakers. Table 4 in this study shows the rate of heart attack in the placebo group was 3.1% while the statin group's rate was 2% — a 36% reduction in relative risk. However, the absolute risk reduction — the actual difference between the two groups, i.e., 3.1% minus 2% — is only 1.1%, which really isn't very impressive. In other words, in the real world, if you take a statin, your chance of a heart attack is only 1.1% lower than if you're not taking it. At the end of the day, what really matters is what your risk of death is the absolute risk. The study, however, only stresses the relative risk (36%), not the absolute risk (1.1%). As noted in the review18 "How Statistical Deception Created the Appearance That Statins Are Safe and Effective in Primary and Secondary Prevention of Cardiovascular Disease," it's very easy to confuse and mislead people with relative risks. You can learn more about absolute and relative risk in my 2015 interview with David Diamond, Ph.D., who co-wrote that paper. Research questioning the veracity of oft-cited statin trials is also reviewed in "Statins' Flawed Studies and Flawed Advertising." Statins Sabotage Your HealthA stunning review of statin trials published in 2015 found that in primary prevention trials, the median postponement of death in those taking statins was a mere 3.2 days. While potentially extending life span by 3.2 days, those taking statins are also at increased risk for:
Oftentimes statins do not have any immediate side effects, and they are quite effective, capable of lowering cholesterol levels by 50 points or more. This is often viewed as evidence that your health is improving. Side effects that develop over time are frequently misinterpreted as brand-new, separate health problems. Crimes Against HumanityThe harm perpetuated by the promotion of the low-fat, low-cholesterol myth is so significant, it could easily be described as a crime against humanity. Ancel Keys' 1963 "Seven Countries Study" was instrumental in creating the saturated fat myth.19,20 He claimed to have found a correlation between total cholesterol concentration and heart disease, but in reality this was the result of cherry picking data. When data from 16 excluded countries are added back in, the association between saturated fat consumption and mortality vanishes. In fact, the full data set suggests that those who eat the most saturated animal fat tend to have a lower incidence of heart disease, which is precisely what other, more recent studies have concluded. Procter & Gamble Co.21 (the maker of Crisco22), the American Heart Association and the Center for Science in the Public Interest (CSPI) all promoted the fallacy for decades, despite mounting evidence that Keys had gotten it all wrong. The AHA was issuing stern warnings against butter, steak and coconut oil as recently as 2017.23 That same year, Procter & Gamble partnered with University Hospitals Harrington Heart & Vascular Institute to promote heart health by lowering cholesterol.24 CSPI was also instrumental in driving heart disease skyward with its wildly successful pro-trans fat campaign. It was largely the result of CSPI's campaign that fast-food restaurants replace beef tallow, palm oil and coconut oil with partially hydrogenated vegetable oils, which are high in synthetic trans fats linked to heart disease and other chronic diseases. As late as 1988, CSPI praised trans fats, saying "there is little good evidence that trans fats cause any more harm than other fats" and that "much of the anxiety over trans fats stems from their reputation as 'unnatural.'"25 CSPI and AHA Omit Their Role in Heart Disease EpidemicToday, you'll have to dig deep to unearth CSPI's devastating public health campaign. In an act of deception, they erased it from their history to make people believe they've been doing the right thing all along. Their historical timeline26 of trans fat starts at 1993 — the year CSPI decided to change course and start supporting the elimination of the same trans fat they'd spent years promoting. 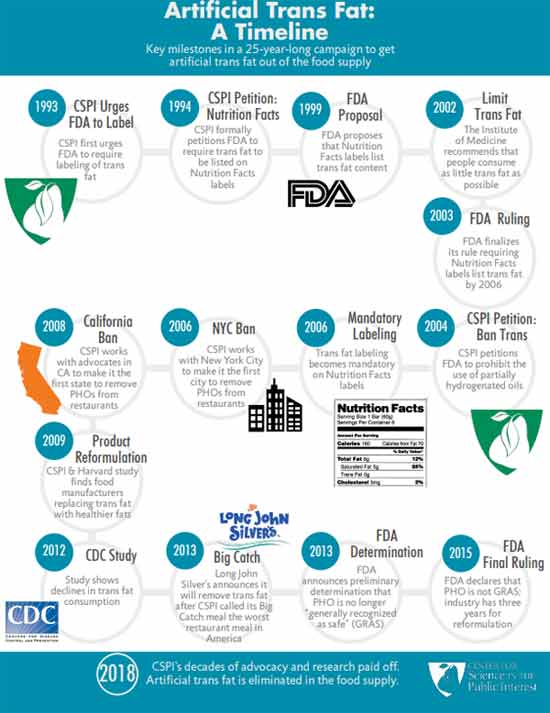
Similarly, the AHA conveniently omits saturated fat and cholesterol from its history of "lifesaving" breakthroughs and achievements.27 It makes sense, though, considering the AHA's and CSPI's recommendations to swap saturated fat for vegetable oils and synthetic trans fat never resulted in anything but an epidemic of heart disease. The idea that the harms of trans fats were unknown until the 1990s is simply a lie. The late Dr. Fred Kummerow started publishing evidence showing trans fat, not saturated fat, was the cause of heart disease in 1957. He also linked trans fat to Type 2 diabetes. You can click on this link to watch my interview with him. I traveled to his home in Urbana, Illinois, shortly before he passed away. The Truth About Saturated FatIn addition to the more recent studies mentioned earlier, many others have also debunked the idea that cholesterol and/or saturated fat impacts your risk of heart disease. For example: • In a 1992 editorial published in the Archives of Internal Medicine,28 Dr. William Castelli, a former director of the Framingham Heart study, stated:
• A 2010 meta-analysis,29 which pooled data from 21 studies and included 347,747 adults, found no difference in the risks of heart disease and stroke between people with the lowest and highest intakes of saturated fat. • Another 2010 study30 published in the American Journal of Clinical Nutrition found that a reduction in saturated fat intake must be evaluated in the context of replacement by other macronutrients, such as carbohydrates. When you replace saturated fat with a higher carbohydrate intake, particularly refined carbohydrate, you exacerbate insulin resistance and obesity, increase triglycerides and small LDL particles, and reduce beneficial HDL cholesterol. According to the authors, dietary efforts to improve your cardiovascular disease risk should primarily emphasize the limitation of refined carbohydrate intake, and weight reduction. • A 2014 meta-analysis31 of 76 studies by researchers at Cambridge University found no basis for guidelines that advise low saturated fat consumption to lower your cardiac risk, calling into question all of the standard nutritional guidelines related to heart health. According to the authors:
Will Saturated Fat Myth Soon Be Upended?To learn more, be sure to listen to Dr. Paul Saladino's interview with Nina Teicholz, previously featured in "Why Chicken Is Killing You and Saturated Fat Is Your Friend." Teicholz, a science journalist, adjunct professor at NYU's Wagner Graduate School of Public Service and the executive director of The Nutrition Coalition, is also the author of "The Big Fat Surprise: Why Butter, Meat and Cheese Belong in a Healthy Diet," which reviews the many myths surrounding saturated fat and cholesterol. In the interview, Saladino and Teicholz review the history of the demonization of saturated fat and cholesterol, starting with Keys, and how the introduction of the first Dietary Guidelines for Americans in 1980 (which recommended limiting saturated fat and cholesterol) coincided with a rapid rise in obesity and chronic diseases such as heart disease. Teicholz also reviews a paper32 in the Journal of the American College of Cardiology, published online June 17, 2020, which actually admits the long-standing nutritional guideline to limit saturated fat has been incorrect. This is a rather stunning admission, and a huge step forward. As noted in the abstract:
from http://articles.mercola.com/sites/articles/archive/2020/08/26/have-statins-reduced-heart-disease.aspx Cardiovascular disease (CVD), or heart disease, is a term that refers to several types of heart conditions. Many of the problems associated with heart disease are related to atherosclerosis. This term refers to a condition in which there's a buildup of plaque along the walls of the artery, making it more difficult for blood to flow and for oxygen to reach the muscles, including the heart. This can be the underlying problem in cases of heart attack, stroke and heart failure. Other types of CVD happen when the valves in the heart are affected or there's an abnormal heart rhythm.1 Heart disease is the leading cause of death in the U.S. and it contributes to other leading causes including stroke, diabetes and kidney disease.2 It also ranks as the No. 1 cause of death around the world: Four out of five deaths are from heart attack or stroke.3 Heart disease accounts for 25% of deaths in the U.S. with a $219 billion price tag, based on data from 2014 to 2015.4 Scientists believe some of the key contributing factors are high blood pressure, smoking, diabetes, physical inactivity and excessive alcohol use. Cholesterol Levels in People Who Had Heart AttacksThere is ongoing disagreement over the levels at which cholesterol presents a risk for heart disease and stroke. Added to this, many doctors and scientists continue to recommend lowering fat consumption and using medications to lower cholesterol levels. A national study from the University of California Los Angeles showed that 72.1% of the people who had a heart attack did not have low-density (LDL) cholesterol levels, which would have indicated they were at risk for CVD. Their LDL cholesterol was within national guidelines and nearly half were within optimal levels.5 In fact, half the patients admitted with a heart attack who had CVD had LDL levels lower than 100 milligrams (mg), which is considered optimal; 17.6% had levels below 70 mg, which is the level recommended for people with moderate risk for heart disease.6 However, more than half the patients who were hospitalized with a heart attack had high-density lipoproteins (HDL) in the poor range, based on a comparison to national guidelines. The team used a national database with information on 136,905 people who received services from 541 hospitals across the U.S. They were admitted between 2000 and 2006 and, while they had their blood drawn upon arrival, only 59% had their lipid levels checked at that time. Of those who were checked, out of everyone who was admitted with a heart attack but didn’t have CVD or Type 2 diabetes, 72.1% had LDL levels less than 130 mg/dL, which was the recommended level at the time of the study (2009). In addition to this, researchers found the levels of HDL cholesterol (the “good” kind) had dropped compared to statistics from earlier years, with 54.6% having levels below 40 mg/dL.7 The desirable level for HDL is 60 mg/dL or higher.8 The findings led researchers to suggest that the guidelines for prescribing cholesterol medication should be adjusted — to lower the number at which drugs should be administered. In other words, they are suggesting that more people be put on cholesterol drugs. As explained by Dr. Gregg C. Fonarow, lead investigator:9
The study was sponsored by the Get with the Guidelines program that's supported by the American Heart Association, which promotes the use of statins for lowering LDL cholesterol.10 Fonarow has done research for GlaxoSmithKline and Pfizer, and has consulted for, and received honoraria from Merck, AstraZeneca, GlaxoSmithKline and Abbott — all of which manufacture cholesterol drugs, including statins. Cholesterol Myth May Be Kept Alive by Big PharmaWhile scientists and physicians continue to investigate the level of cholesterol that may affect heart attack risk, the theory that dietary cholesterol is a contributor has long been proven false. In the 1960s it may have been a conclusion that researchers made based on the available science, but decades later the evidence does not support the hypothesis.11 Yet, as some researchers have pointed out, the move toward removing dietary cholesterol limits has been slow. In the past 10 years, some have modified recommendations to address certain negative consequences of limiting dietary cholesterol, such as the risk of having inadequate levels of choline. Unfortunately, others have continued to promote low-fat diets and that could have hazardous results. Whether discussing cholesterol intake or serum cholesterol levels, the data do not support the hypothesis that it relates to heart disease. I believe it appears that the evidence supporting the use of cholesterol-lowering statin drugs is likely little more than the manufactured work of pharmaceutical companies. This also appears to be the conclusion of the authors of a scientific review published in the Expert Review of Clinical Pharmacology.12 The team identified significant flaws in three recent studies: “… large reviews recently published by statin advocates have attempted to validate the current dogma. This article delineates the serious errors in these three reviews as well as other obvious falsifications of the cholesterol hypothesis.” The authors present substantial evidence that total cholesterol and LDL cholesterol are not indicators of heart disease risk. In addition, statin treatment is doubtful as a form of primary prevention. In their analysis, they point out that if high cholesterol levels were a major cause of atherosclerosis, patients with high total cholesterol whose levels were lowered the most by statin drugs should see the greatest benefit. However, evidence does not show that to be the case. In another review of statin trials and other studies in which cholesterol was linked to heart disease, researchers could not find a correlation between cholesterol and the degree of coronary atherosclerosis, coronary calcification or peripheral atherosclerosis. They found no exposure response in which those with the highest level of cholesterol enjoyed the greatest benefit from reduction.13 These researchers propose the link between high LDL or total cholesterol and heart disease may be secondary to other factors that promote CVD, such as:14
Saturated Fat Is Crucial but Vegetable Oil Is DeadlyOne of the reasons so many people are sick is that we’re constantly told that animal fats are unhealthy and industrial vegetable oils are not, and people believe it. The authors of a recent paper in the Journal of the American College of Cardiology admits the long-standing nutritional guideline to limit saturated fat is incorrect. This is a tremendous step forward in righting a dietary wrong that started with Ancel Keys’ flawed hypothesis15 and has since had a significant impact on health and wellness. As the researchers note in the abstract:16
In a recent speech at the Sheraton Denver Downtown Hotel, titled "Diseases of Civilization: Are Seed Oil Excesses the Unifying Mechanism?" Dr. Chris Knobbe revealed evidence that seed oils, so prevalent in modern diets, are the reason for most of today's chronic diseases.17 His research charges the high consumption of omega-6 seed oil in everyday diets as the major unifying driver of the chronic degenerative diseases so prevalent in modern civilization. He calls the inundation of Western diets with harmful seeds oils "a global human experiment … without informed consent." You’ll find more, including a video of his presentation in “Are Seed Oils Behind the Majority of Diseases This Century?” Your Omega-3 Index Is More Predictive Than CholesterolThe combination of a diet high in omega-6 fats commonly found in vegetable oils and low in omega-3 fats, commonly found in fatty fish, is yet another risk factor for coronary heart disease. As the National Institutes of Health describes:18
Each of the three fats plays a unique role in cellular health. The authors of one study analyzed the risk of a cardiovascular event while taking icosapent ethyl.19 The medication is a "highly purified omega-3 fatty acid" that is "a synthetic derivative of the omega-3 fatty acid eicosapentaenoic acid (EPA)."20 Those who took the medication had a significantly lower number of ischemic events than those taking the placebo. An omega-3 deficiency leaves you vulnerable to chronic disease and lifelong challenges. The best way to determine if you're getting enough is to be tested, as it’s a good predictor of all-cause mortality.21 The omega-3 index is a measure of the amount of EPA and DHA in red blood cell membranes. This has been validated as a stable and long-term marker because it reflects your tissue levels. An index greater than 8% is associated with the lowest risk of death, while an index lower than 4% places you at the highest risk of heart disease-related mortality.22 Your best sources of fatty fish are wild-caught Alaskan salmon, herring, mackerel and anchovies. The larger predatory fish, such as tuna, have much higher amounts of mercury and other toxins. It's important to realize your body can’t convert enough plant-based omega-3 to meet your needs. That means that if you're a vegan, you must figure out a way to compensate for the lack of marine or grass fed animal products in your diet. If your test results are low, and you are considering a supplement, compare the advantages and disadvantages of fish oil and krill oil. Krill are wild-caught and sustainable, more potent than fish oil and less prone to oxidation. You’ll find more about the benefits of maintaining adequate levels of omega-3 fats in “Omega-3 Index More Predictive Than Cholesterol Levels.” Know Your Cholesterol RatiosThe cholesterol myth has been a boon to the pharmaceutical industry since cholesterol-lowering statins have become some of the more frequently prescribed and used drugs. In a report by the U.S. Preventive Services Task Force published in JAMA, evidence showed that 250 people need to take a statin drug for one to six years to prevent one death from any cause.23 When measuring cardiovascular death specifically, 500 would have to take a statin drug for two to six years to prevent even one death. As the evidence mounts that statin drugs are not the answer and simple cholesterol levels may not help you understand your risk of heart disease, it's time to use other risk assessments. In addition to an omega-3 index, you can get a more accurate idea of your risk of heart disease using an HDL/total cholesterol ratio, triglyceride/HDL ratio, fasting insulin level, fasting blood sugar level and iron level. You’ll find a discussion of the tests and measurements in “Cholesterol Does Not Cause Heart Disease.” from http://articles.mercola.com/sites/articles/archive/2020/08/26/cholesterol-levels-in-people-who-had-heart-attacks.aspx Late in May 2020, media producer Mikki Willis released the first part of his documentary “Plandemic,” featuring Judy Mikovits, Ph.D., a cellular and molecular biologist1 whose research revealed many vaccines are contaminated with gammaretroviruses, due to the viruses being grown in contaminated animal cell lines. The 26-minute film was banned on every social media platform after going viral.2 August 18, 2020, Part 2, titled “Plandemic — Indoctornation,” was released. Plandemic — IndoctornationPart 2 is a full-length feature, revealing the driving force behind the vaccine agenda. It looks at the roles of the World Health Organization, Bill Gates, Tedros Adhanom, Dr. Anthony Fauci, mainstream media, Silicon Valley tech giants, Big Pharma and many others, connecting the dots between them. Willis interviews a variety of individuals, including:
Free supplemental footage, including a follow-up interview with Mikovits, as well as links to additional resources provided by all of the interviewees are supposed to be available on the film’s website, plandemicseries.com. Event 201The film starts out by reviewing Event 201, a pandemic preparedness simulation hosted by the Johns Hopkins Center for Health Security, the World Economic Forum and the Bill and Melinda Gates Foundation in October 2019 — 10 weeks before the COVID-19 outbreak first began in Wuhan. This scripted tabletop exercise included everything we now see playing out in real time, in the real world, from PPE shortages, lockdowns and removal of civil liberties to mandated vaccination campaigns, riots, economic turmoil and the breakdown of social cohesion. A highlight reel of the predictions put forth during this event is included in the documentary. At the time, they spent a great deal of time discussing ways to limit and counter the spread of expected “misinformation” about the pandemic and the vaccines that would have to be developed. In addition to outright censorship, their plan included the use of “soft power,” a term referring to stealth influencing using celebrities and other social media influencers. I discussed this in “The PR Firm Behind WHO’s Celeb Endorsements.” Just as in real life, one of the pieces of “misinformation” that had to be countered was rumors that the virus had been created and released from a bioweapons laboratory. Operation Mockingbird Never Ended, It Just Got PrivatizedThe film also reveals how SARS-CoV-2 has been turned into a profit center, the possible origins of SARS-CoV-2, and how Silicon Valley tech giants are controlling the narrative, pushing fearmongering and censoring differing views. What we’re seeing is straight out of the Operation Mockingbird playbook, a clandestine CIA media influencing campaign launched in the 1950s. During the Cold War, the CIA used it to spread propaganda. It recruited journalists to pen fake stories that disparaged communist ideologies. Today, they’re doing the complete opposite, promoting radical socialist ideas that support their plan for a technocratic economic system. As revealed in the widely-banned documentary “Shadowgate,”3,4 a shadow government has built up behind the scenes, and they’re using sophisticated psychological warfare tools against the American public to further their nefarious agenda. Shockingly, the reason this shadow government — led by government contractors, privatized intelligence companies — are able to manipulate public opinion is because they’ve been illegally siphoning the data collected by the NSA from all Americans, and privatizing it. All of our personal data, combined with artificial intelligence and so-called localization strategies, allows sophisticated computer programs to predict which action or public message will result in a particular outcome. We’re in the midst of a social engineering project that poses a serious existential threat to our personal liberty and freedom. We’re all exposed to it daily, and have been for years. It’s just that now it’s become so pervasive, it’s blatantly obvious for anyone willing to see it. As you’d expect, “Plandemic — Indoctornation” also spends some time reviewing the role of Bill Gates and his foundation. CDC Owns Coronavirus PatentsWillis interviews David E. Martin, Ph.D., a national intelligence analyst and founder of IQ100 Index, which developed linguistic genomics, a platform capable of determining the intent of communications. According to Martin, in 1999, IBM digitized 1 million U.S. patents, which allowed his company to conduct a review. Using linguistic genomics technology, Martin made the “horrific assessment” that one-third of all patents filed in the U.S. were functional forgeries, meaning that “while they had linguistic variations, they covered the same subject matter.” In 1999, patents for coronavirus also started to appear, “and thus began the rabbit trail,” Martin says. In 2003, Asia experienced an outbreak of SARS. Almost immediately, scientists began racing to patent the virus. Ultimately, the U.S. Centers for Disease Control and Prevention nabbed ownership of SARS-CoV (the virus responsible for SARS) isolated from humans. The CDC actually owns the entire genetic content of that SARS virus. It’s patented under U.S. patent 7776521. They also own patents for detection methods, and for a kit to measure the virus. U.S. patent 7279327,5 filed by the University of North Carolina at Chapel Hill, describes methods for producing recombinant coronaviruses. Ralph Baric, Ph.D., a professor of microbiology and immunology who is famous for his chimeric coronavirus research, is listed as one of the three inventors, along with Kristopher Curtis and Boyd Yount. According to Martin, Fauci, Baric and the CDC “are at the hub” of the COVID-19 story. “In 2002, coronaviruses were recognized as an exploitable mechanism for both good and ill,” Martin says, and “Between 2003 and 2017, they [Fauci, Baric and CDC] controlled 100% of the cash flow to build the empire around the industrial complex of coronavirus.” CDC Has Broken the Law, One Way or AnotherNow, here’s the key take-home message Martin delivers. There’s a distinct problem with the CDC’s patent on SARS-CoV isolated from humans, because, by law, naturally occurring DNA segments are prohibited from being patented. The law clearly states that such segments are “not patent eligible merely because it has been isolated.” So, either SARS-CoV was manmade, which would render the patent legal, or it’s natural, thus rendering the patent on it illegal. However, if the virus was manufactured, then it was created in violation of biological weapons treaties and laws. This includes the Biological Weapons Anti-Terrorism Act of 1989, passed unanimously by both houses of Congress and signed into law by George Bush Sr., which states:6
So, as noted by Martin, regardless of which scenario turns out to be true, the CDC has broken the law one way or another, either by violating biological weapons laws, or by filing an illegal patent. Even more egregious, May 14, 2007, the CDC filed a petition with the patent office to keep their coronavirus patent confidential. Now, because the CDC owns the patent on SARS-CoV, it has control over who had the ability to make inquiries into the coronavirus, Martin notes. Unless authorized, you cannot look at the virus, you cannot measure it or make tests for it, since they own the entire genome and all the rest.
Dangerous Gain-of-Function Research Was PermittedMartin goes on to describe events occurring between 2012 and 2013. At that time, the National Institutes of Health decided to take another look at gain-of-function research, ultimately deciding that gain-of-function research on coronavirus was too risky to continue. This led to the suspension of funding of such research in 2013. That included funding flowing into Harvard, Emery and University of North Carolina Chapel Hill. However, while the NIH had moral and even legal reasons for suspending such research, they made the funding pause voluntary, not mandatory. Then, in 2014, when the push-back against gain-of-function research into coronaviruses grew further, the NIH — under the leadership of Fauci — offshored that research to — you guessed it — the Wuhan Institute of Virology in China. However, as detailed by Martin, the funding was not sent in a straight-forward way. Instead, it was funneled through front organizations such as the EcoHealth Alliance, led by its president, Peter Daszak, whose research, according to the EchoHealth Alliance website, “includes identifying the bat origin of SARS.”7 Between 2014 and 2019, EcoHealth Alliance received a long list of grants from the NIH to study “the risk of bat coronavirus emergence.” EcoHealth Alliance then subcontracted that work to the Wuhan Institute of Virology. So, in the end, the U.S. could deny culpability, blaming the outbreak on China when, in fact, it was American research that had been outsourced. Interestingly, in late-breaking news August 19, 2020, The Wall Street Journal8 reported that the NIH had notified EcoHealth that it wants “a sample of the new coronavirus that the Wuhan researchers used to determine its genetic sequence,” along with study details and other information. Additionally, the NIH demanded that EcoHealth “arrange for an inspection of the Wuhan Institute of Virology by an outside team that would examine the facility’s lab and records ‘with specific attention to addressing the question of whether WIV staff had SARS-CoV-2 in their possession prior to December 2019.’” The problem, Martin notes in “Indoctornation,” is that while the evidence is staring us right in the face, we’re told that so-called “fact-checkers” have a transcendent view of the situation, and they are the ultimate arbiters of truth. As a result, we have this very strange situation where facts and logic are being steamrolled and lambasted as good old-fashioned heresy. Will Truth Prevail?The film goes on to interview many other experts, many of whom are convinced the evidence points to SARS-CoV-2 being a manmade virus. Like Plandemic Part 1, Part 2 is well worth your time. As noted by Willis, in today’s fast-paced world, few have the time to do the necessary research to unveil what’s really going on. The evidence is there, but you have to put it together. This is why documentaries such as “Plandemic” and “Shadowgate” are so useful. They weave the dots together so that you can see a fuller, more complete picture. Unfortunately, the picture at present is grim. Yet, we must face it because it’s not going away or resolving in the near future. It is important to understand that we are all being subjected to a massive propaganda campaign to move us toward a very specific technocratic agenda. It is only by seeking alternative views that we can begin to understand the truth. In the case of coronavirus, it should be clear that gain-of-function research is a dangerous game that should not be permitted. By giving researchers the go-ahead to continue this kind of research, even as the NIH publicly “paused” funding for it, the NIH failed to uphold its moral and legal responsibilities. It’s also clear that the CDC has engaged in illegal activities relating to the patenting of the virus, and that they had ample motive and means to profit from a coronavirus pandemic. It’s hard to imagine a more corrupt system than what we currently have. The question is: When will something be done about it? from http://articles.mercola.com/sites/articles/archive/2020/08/25/plandemic-indoctornation.aspx This Mercury Awareness Week we celebrate the 20th anniversary of Consumers for Dental Choice, the nonprofit advocacy wing of the mercury-free dentistry movement. It is also our 10th Mercury Awareness Week, during which we step forward to educate the public and empower dentists to choose mercury-free dentistry, and when I put my resources to support Charlie Brown and his team by matching every dollar you donate. Thanks to your donations, Consumers for Dental Choice has gone a long way toward taking mercury-free dentistry from dream to reality. I ask that you continue your support by donating at ToxicTeeth.org, and I will double your gift all of this week, August 23 to 29, 2020 (up to $150,000). So, here's your chance to double your impact for mercury-free dentistry!
Together, we can finish making the dream of mercury-free dentistry a reality, building on Consumers for Dental Choice's track record of victories in the states, at the federal level and worldwide. Supporting Mercury-Free Dentists, Protecting Patients' RightsWhen Consumers for Dental Choice started, mercury-free dentists were under attack by their state dental boards. These boards were stacked with pro-mercury dentists recommended for the appointment by pro-mercury dental associations. And of course, the pro-mercury dentists had a strong interest in stripping their mercury-free dentist competition of their licenses — and that is just what they did. So, Consumers for Dental Choice challenged those tyrannical dental boards — and won. Charlie Brown, who was twice elected Attorney General of West Virginia, struck down the boards' gag rule that prevented dentists from advising, advocating and advertising mercury-free dentistry. Not only did he block boards from taking dental licenses, but he even won back dental licenses in California and Iowa. Then Consumers for Dental Choice went on the offensive. This nonprofit group succeeded in getting mercury-free dentists appointed or reappointed to dental boards in California, Minnesota and Washington state. And then it got several states — Maine, Connecticut, California and New Hampshire, as well as the city of Philadelphia — to pass laws that require dentists to distribute fact sheets telling patients that amalgam is made of mercury and that non-mercury alternatives are available. When the California dental board refused to produce a fact sheet as required by the law, Consumers for Dental Choice helped get the board disbanded. A new dental board, one that would follow the law requiring it to develop a fact sheet, was appointed. Now Consumers for Dental Choice has returned to the state with a vengeance — turning the tables on state dental boards: 1. Consumers for Dental Choice Challenged the Maine Dental Board -- The Board's backroom tactics supporting mercury fillings led Charlie to file an antitrust petition with the Federal Trade Commission. The dental board either saw the light or felt the heat — it's pretty easy to see which — and adopted a new regulation, which took effect during the pandemic:
As you can see, the word "mercury" — the term the ADA tried to hide for a century — is mentioned multiple times in this rule. 2. Petition Filed to the State of Connecticut Dental Board -- The state of Connecticut has a fact sheet law but refuses to enforce it. Additionally, its Medicaid program mandates only mercury fillings for adults (limiting consumer choice) and excludes mercury-free dentists from participation (limiting consumer access to dental care). In July 2020, Consumers for Dental Choice, joined by the Connecticut Coalition for Environmental Justice and the Mercury Policy Project, filed both a petition to the dental board and a complaint to the state attorney general. 3. Petition Filed to Ban Sales of Amalgam for Children in Wisconsin -- The state of Wisconsin has a rule banning sales of products or other articles aimed at children that contain mercury. Using diligent research to find this little-noticed regulation, Consumers for Dental Choice and its Wisconsin allies filed a petition in August 2020 to ban sales of amalgam for children. US Regulators Now Engaging Mercury-Free Dentistry MovementArmed with its victories at the state level, Consumers for Dental Choice took on the federal government. For three decades, the U.S. Food and Drug Administration (FDA) had been dodging its duty to classify — that is, issue a rule for — amalgam. Consumers for Dental Choice took action. After assembling plaintiffs, Consumers for Dental Choice sued the FDA to classify amalgam in 2008. The judge agreed and told the FDA to sit down with Consumers for Dental Choice to determine a deadline. FDA was compelled to commit to classifying amalgam by July 2009. But when July 2009 came around it was clear the FDA had not considered the science in its abysmal rule. Now Consumers for Dental Choice has convinced FDA to re-open its rule, as I will detail in another article coming on August 27, 2020. Teaming with other environmental groups, Consumers for Dental Choice challenged the EPA to require pro-mercury dentists to install and maintain amalgam separators, a device that can capture some of amalgam's mercury before it enters wastewater. After multiple meetings, a congressional hearing and petitions, EPA finally issued a separator rule. Consumers for Dental Choice didn't stop with these federal regulators. It went to the State Department, calling for the U.S. government to take a stand for mercury-free dentistry at the negotiations for the mercury treaty that would come to be known as the Minamata Convention on Mercury. In the end, the U.S. government became a party to the Minamata Convention, supporting this treaty's required reduction of amalgam use. In these ways, Consumers for Dental Choice took the federal government from doing nothing to having to face the amalgam issue head-on. Amalgam Bans and Restrictions Now a Worldwide PhenomenonConsumers for Dental Choice launched its international campaign in 2010 by establishing the World Alliance for Mercury-Free Dentistry, a coalition of environmental, patient and dental organizations dedicated to phasing out amalgam use. At that time, only two countries had banned amalgam use: Sweden and Norway. And no one thought other countries — especially developing countries — could replicate this success. But Consumers for Dental Choice dug in, and the coalition it assembled dug in. They ignited campaigns around the world — including workshops, stakeholder meetings, conferences with government officials, written submissions, petitions, grassroots organizing and outreach to dental schools, dental associations and dental professionals. All of that work paid off, and now amalgam bans and restrictions are more and more common all over the world. Check out the video at the top of the article to learn more about these victories, including these highlights:
With Consumers for Dental Choice's help, the number of countries banning and restricting amalgam use has grown exponentially, especially in the past few years as even developing countries are successfully phasing out and restricting amalgam use. Now Consumers for Dental Choice is building on this international momentum to end amalgam use in North America, too. Taking Mercury-Free Dentistry From Dream to RealityConsumers for Dental Choice has taken the dream of mercury-free dentistry a long way — and you can help this effective advocacy organization finish making it a reality for all people, everywhere. Will you consider a donation to this 501(c)(3) nonprofit organization dedicated to advocating mercury-free dentistry? I will match all donations during Mercury-Free Dentistry Week (August 23 to 29, 2020) up to $150,000. Donations are tax-deductible and can be made online at ToxicTeeth.org. Checks can be mailed to: Consumers for Dental Choice Thank you for helping make the dream of mercury-free dentistry into reality!
And remember, you don't need to wait to make mercury-free dentistry a reality for you and your children — you can choose a mercury-free dentist right now. Check out Consumers for Dental Choice's listing of mercury-free dentists now. from http://articles.mercola.com/sites/articles/archive/2020/08/25/consumers-for-dental-choice-banish-dental-amalgam.aspx Quercetin was initially found to provide broad-spectrum protection against SARS coronavirus in the aftermath of the SARS epidemic that broke out across 26 countries in 2003.1,2,3 Now, some doctors are advocating its use against SARS-CoV-2, in combination with vitamin C, noting that the two have synergistic effects. Incidentally, ascorbic acid (vitamin C) and the bioflavonoid quercetin (originally labeled vitamin P) were both discovered by the same scientist — Nobel prize winner Albert Szent-Györgyi.4,5 Quercetin’s antiviral capacity has been attributed to five main mechanisms of action:
Similarly, vitamin C at extremely high doses also acts as an antiviral drug, effectively inactivating viruses. During the 2003 SARS pandemic, a Finnish researcher called6 for an investigation into the use of vitamin C after research showed it not only protected broiler chicks against avian coronavirus, but also cut the duration and severity of common cold in humans and significantly lowered susceptibility to pneumonia. The MATH+ ProtocolWhile high-dose vitamin C is new for COVID-19 treatment, it’s been used as a treatment for sepsis since about 2017. The vitamin C-based sepsis treatment was developed by Dr. Paul Marik, a critical care doctor at Sentara Norfolk General Hospital in East Virginia, which has since adopted it as standard of care for sepsis. In the interview above, Marik explains how the COVID-19 critical care protocol grew out of his sepsis treatment, as he and other doctors noticed there were many similarities between sepsis and severe COVID-19 infection, in particular the out-of-control inflammatory cascade. To address the differences between the two conditions, a group of doctors, including Marik, founded the Front Line COVID-19 Critical Care Working Group7 (FLCCC), and began developing a modified protocol specifically for COVID-19. The original protocol for COVID-19 is detailed in “COVID-19 Critical Care.” Known as the MATH+ protocol,8,9 it involves the use of three key medicines, all of which need to be started within six hours of hospital admission:
MATH+ Prophylactic and At-Home Treatment ProtocolThe initial MATH+ protocol10 was released in April 2020. In early July and August, it was updated11,12 to include quercetin and a number of optional nutrients and drugs, not only for critical care but also for prophylaxis and mild disease being treated at home. For prophylaxis, the FLCCC recommends:13
The at-home treatment for mildly symptomatic patients is very similar, but adds several optional drugs, including aspirin (ASA), famotidine (an antacid), ivermectin (a heartworm medication that has been shown to inhibit SARS-CoV-2 replication in vitro14). (For dosages, see the Critical Care Management Protocol15 summary, available on the Easter Virginia Medical School’s site.) They also recommend monitoring your oxygen saturation with a pulse oximeter and to go to the hospital if you get below 94%. The medical evidence to support each drug and nutrient can be found under “Medical Evidence”16 on the FLCCC’s website. MATH+ Critical Care In-Hospital ProtocolIn July, the in-hospital protocol was revised17 again to include thiamine (which is also a key ingredient in Marik’s sepsis protocol). As of the last revision, the in-hospital MATH+ protocol18 calls for:
According to the FLCCC, “By initiating the protocol soon after a patient meets criteria for oxygen supplementation, the need for mechanical ventilators and ICU beds will decrease dramatically.” While heparin is an important part of the protocol due to the clotting complications in the microvasculature of the lung, it is likely that N-acetyl cysteine (NAC) is likely a far better choice as it is far safer and likely as effective. The Two Phases of Disease Require Different TreatmentsThis is a key point: There are two distinct phases or stages of COVID-19 — the viral replication stage and the immune dysfunction stage — and the treatment must be appropriate for the stage you’re in. Equally crucial is starting aggressive treatment as early as possible. The graphic below details the two stages of disease, and the FLCCC’s suggested treatment focus for each. Peak viral replication takes place at the earliest signs of symptoms, which include cold/flu-like symptoms, loss of taste and smell, myalgia (muscle pain) and general malaise. From the time of symptom onset to the time that immune dysregulation starts to set in (accompanied by worsening symptoms) is about five or six days. During this time, you need to aggressively treat, whether you’re at home (see the at-home treatment for symptomatic patients) or in the hospital. The key remedies in this phase are antivirals (which is what vitamin C, quercetin and zinc are). Anti-inflammatories should be avoided in this phase, Marik warns. Again, if treating at home, be sure to monitor your oxygen saturation with a pulse oximeter. If your oxygen drops to 94% or below when sitting or walking, it’s time to go to the hospital. If your immune system is unable to successfully combat the virus, then five to six days after first symptoms, early pulmonary dysfunction can set in. At this point, anti-inflammatories — i.e., corticosteroids — and immune suppressive therapeutics are required. 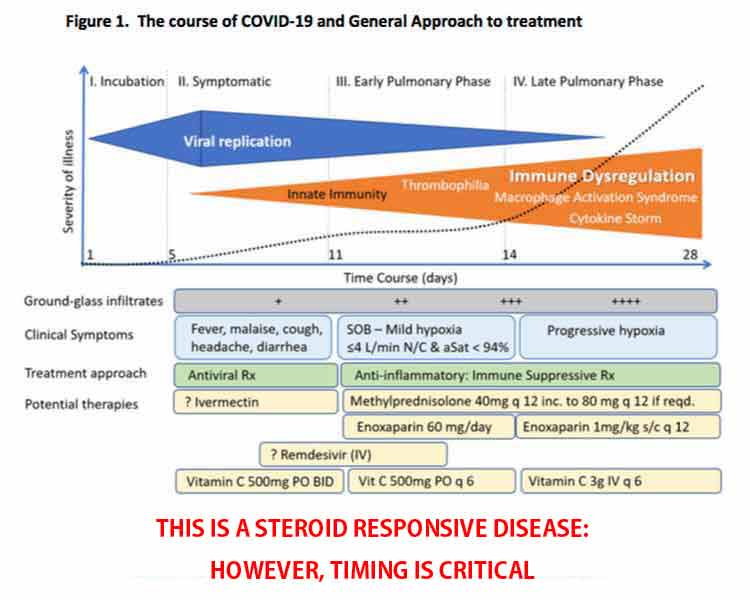
Viral Load Declines as Inflammation RisesAnother important concept explained by Marik in the featured interview is that the inflammatory response rises as the viral load decreases. They do not rise together. “So, it’s really not the virus that is causing cytopathic effects,” he says. By the time you enter the pulmonary phase of the disease, your viral load has actually significantly decreased, but for some reason the inflammatory response then starts to run amok. Your oxygen saturation is “the key indicator of pulmonary involvement,” Marik says. Once your oxygen saturation starts to decline, you are entering the early pulmonary phase where inflammation is rapidly increasing. This is why it’s so important to make sure you’re measuring your oxygen saturation. Do not try to treat at home if your oxygen is dropping. Go to the hospital. Again, early treatment is crucial. Hopefully, your doctor will be willing to implement the MATH+ protocol. Corticosteroids Are a Crucial ComponentIn a short essay19 co-written by the entire FLCCC team, they express their conviction that the MATH+ protocol is one of the best, most effective, critical care protocols for COVID-19 to date.
The essay20 stresses the importance of corticosteroids in the treatment of COVID-19, and cites results from the RECOVERY trial,21,22,23 a large, randomized controlled COVID-19 study by the University of Oxford, that validates their recommendation to use corticosteroids as soon as the patient is hospitalized. In that study, the corticosteroid dexamethasone improved survival by one-third in ventilated patients and one-fifth in those requiring oxygen. However, the FLCCC believes another type of corticosteroid, methylprednisolone, is a better, more effective, choice. First, because it reaches higher concentrations in lung tissue, and secondly, because it most closely matches the inflammatory gene activation patterns induced by SARS-CoV-2. They also believe the dexamethasone dose used in the RECOVERY trial was too low, especially for severe cases.
Vitamin C and Quercetin Work SynergisticallyJune 19, 2020, Marik published the paper,25 “Quercetin and Vitamin C: An Experimental, Synergistic Therapy for the Prevention and Treatment of SARS-CoV-2 Related Disease (COVID-19)” in the journal Frontiers in Immunology, which notes:
The paper presents evidence for the use of vitamin C and quercetin — based on their biological actions and pharmacokinetics profiles — both as prophylaxis in high-risk populations, and as an adjunct to drugs such as Remdesivir or convalescent plasma in the treatment of hospitalized COVID-19 patients. Post-COVID SyndromeIn the interview, Marik also addresses the issue of “post-COVID syndrome,” which he says is very similar to that of post-sepsis syndrome. In some cases, COVID-19 patients have recovered from the infection, only to die due to pulmonary embolism (blood clots in the lungs) or other organ dysfunction. Marik suspects this is because the inflammatory response is still overactive. Many sepsis patients will have very high cytokine levels even a year after their recovery. He believes steroids are one key to downregulating the inflammatory response, which would prevent this problem. A good way to screen for this, Marik says, is to measure CRP, which appear to be a good marker for ongoing inflammation. If CRP is high after recovering from COVID-19, Marik suggests doing a short course of corticosteroids to downregulate the inflammatory response. Aspirin may also be helpful if D-dimer is high. These should be used under medical supervision. I believe this information needs to be shared far and wide, if we are to prevent more people from dying unnecessarily. More and more, as doctors are starting to speak openly about their clinical findings, we see there are quite a few different ways to tackle this illness without novel antivirals or vaccines, using older, inexpensive and readily available medications and nutrients that are already known to be safe. from http://articles.mercola.com/sites/articles/archive/2020/08/24/quercetin-and-vitamin-c-synergistic-effect.aspx 1 Which of the following organizations conducted a highly successful campaign promoting trans fat in the 1980s, resulting in an epidemic of heart disease? 2 Which former FDA commissioner now sits on the board of directors at Pfizer, which was granted a $1.95 billion deal with the U.S. government to provide Americans with 100 million doses of its COVID-19 vaccine? 3 According to mounting scientific evidence, SARS-CoV-2, responsible for COVID-19 disease, spreads via contact with contaminated surfaces (fomites): 4 A "COVID-19 case" refers to: 5 Which of the following foundations is presently the largest funder of the World Health Organization if the U.S. holds good on withdrawing its WHO funding? 6 According to an analysis by the U.S. Department of Health and Human Services Agency for Healthcare Research Quality of health data collected from 376,452 individuals who received a total of 1.4 million doses of 45 vaccines, vaccine injuries occur in: 7 Which of the following is a significant source of environmental mercury pollution? from http://articles.mercola.com/sites/articles/archive/2020/08/24/week-144-health-quiz.aspx July 15, 2020, the Dietary Guidelines Advisory Committee (DGAC) published its 2020 report, an independent scientific review on the nutrition and health status of Americans, and there was a concerning finding: Most Americans don't get enough choline, an essential nutrient that's vitally important, but rarely discussed. Marie Caudill, Ph.D., a registered dietitian who is internationally recognized for her research on choline and folate, says the most alarming find from the report is that the populations who would benefit the most from extra choline — pregnant and lactating women, infants and children — are falling especially short. In pregnant women, choline deficiency is associated with an increased risk of neural tube defects. In the general population, getting too little choline can lead to the development of nonalcoholic fatty liver disease and muscle damage. What Does Choline Do?Choline is often lumped in with the B vitamins, but it's not technically a vitamin. It's more of a vitamin-like nutrient.1 Choline helps support optimal health at all stages of life. It plays a role in healthy fetal development, helps maintain cognition and memory, boosts energy, improves fitness and keeps your liver healthy. Your brain and nervous system need adequate amounts of choline to help regulate muscle control, mood and memory.2 Choline is also involved in metabolism. Other roles of choline include:
The Problems With Choline DeficiencyIf you don't get enough choline through your diet, it can result in a choline deficiency, which has widespread negative health effects. Because choline is involved in fat metabolism, low levels of the nutrient can result in an overaccumulation of deposits of fat in your liver.19 Eventually, this can lead to nonalcoholic fatty liver disease and nonalcoholic steatohepatitis, which currently affect 30% of the U.S. population.20 Choline deficiency can also lead to liver damage and muscle damage.21 Choline deficiency can be even more worrisome for pregnant women and lactating mothers. Choline is essential for proper brain development of a growing fetus. It also helps maintain proper homocysteine concentrations during pregnancy.22 According to a study published in the American Journal of Epidemiology, there is an increased risk of neural tube birth defects in babies of women who consume less than 300 mg of choline per day when compared to pregnant women who get at least 500 mg daily.23 Because choline will be pulled from the mother's blood to supply adequate amounts to the fetus, pregnant and lactating women have higher choline needs, yet only 5% get enough, according to one study.24 In addition to pregnant and lactating women, groups at especially high risk for choline deficiency include:
How Much Choline Do You Need?Your liver makes some choline, but the amount isn't enough to keep you healthy and prevent the adverse effects of choline deficiency. That's why you need to get adequate amounts through your diet. The amount of choline you need depends on your age, sex and whether or not you're pregnant or nursing. Here's a general breakdown from the National Institutes of Health30:
Keep in mind, however, that some people have genetic polymorphisms that increase the need for choline and certain ethnic and racial groups are more likely to be affected.31 According to Chris Masterjohn, who has a Ph.D. in nutritional science, eating a diet that's high in (otherwise healthy) saturated fats can also increase your need for choline.32 How to Get More CholineGrass fed beef liver is the richest dietary source of choline, with 430 mg of choline per 100-gram cooked serving.33 But liver isn't as much a staple on American plates as the second highest source of choline — eggs. One single egg, which weighs around 50 grams, contains 169 mg of choline.34 Here's the catch, though: Most of that choline, or 139 mg, is found in the yolk.35 Egg yolks are also rich in lecithin, a fatty acid that's a precursor for choline. That means if you're still following the outdated and totally misguided advice to eat only the egg whites, you're missing out on a lot of the egg's nutrition. Krill oil, which comes from krill, a crustacean mainly eaten by whales, penguins and other aquatic creatures, is also a rich source of choline. A 2011 study published in the journal Lipids found 69 choline-containing phospholipids in krill oil.36 Of those phospholipids, 60 were phosphatidylcholine substances, which protect against liver disease (including hepatitis and cirrhosis in alcoholics), reduce digestive tract inflammation and lessen symptoms associated with inflammatory conditions such as ulcerative colitis and irritable bowel syndrome.37 Other dietary sources of choline include:38
According to the DGAC, most multi-vitamin supplements don't contain sufficient amounts of choline. You can find supplements that contain only choline, but it's always best to try to get what you need through a healthy diet. from http://articles.mercola.com/sites/articles/archive/2020/08/24/choline-deficiency.aspx For the 10th consecutive year, we now celebrate our annual Mercury Awareness and Mercury-Free Dentistry Week. With us again is Charlie Brown, executive director of Consumers for Dental Choice and former attorney general for West Virginia. As in previous years, during this week of August 23 through 29, 2020, we will double your donations to Consumers for Dental Choice, matching it dollar for dollar up to $150,000. I’m committed to doing this annual fundraiser because eliminating dental mercury is such an important effort for both human and environmental health. Over 20 years ago, Brown committed his life to this advocacy, to help improve the lives of millions of people, and your generous donations are what allow him to continue this crucial humanitarian work.
He’s made great progress this past year, which he details in this interview. You will be delighted to know your past donations have been put to good use, and it is thanks to you that this stellar nonprofit group has been able to have such a sustained impact. This has in part been accomplished through the founding of the World Alliance for Mercury-Free Dentistry, a coalition of nonprofit groups from all over the world, which elected Charlie Brown as its president. As explained by Brown:
International ProgressInternationally, the World Alliance for Mercury-Free Dentistry’s success in including amalgam as a plank at the Minamata Convention on Mercury — a global treaty to protect human health and the environment from the adverse effects of mercury signed in 2013 that went into effect in 2017 — has led to actions by governments across the world. Notably, the 27-nation European Union in 2018 banned dental amalgam in children under 15 and in pregnant or breastfeeding women. Health Canada also passed guidelines years ago against the use of amalgam in children, pregnant women and in those with kidney disease but, regrettably, Health Canada seems to have lost interest in using its own guidelines. Ten governments have gone further and implemented either immediate bans or a precise phase-out date. In the past year, the Philippines, Ireland, Nepal, Slovakia, Finland, New Caledonia, Moldova and the Czech Republic have all joined Norway and Sweden in the winner’s circle. It gets better: At the third Conference of the Parties of the Minamata Convention in Geneva in November 2019, all Parties to the treaty (well over 100 countries, including the U.S. and Canada) were instructed to redouble efforts and accelerate the phase-down of amalgam. To facilitate the global phase-out of amalgam, the World Alliance for Mercury-Free Dentistry helped create centers to coordinate the implementation of mercury-free dentistry in each region. There’s the Asian Center for Environmental Health in Bangladesh, the European Center for Environmental Medicine in Berlin, the African Center for Environmental Health in the Ivory Coast, and the Latin American Center for Environmental Health in Uruguay. A specialized campaign is tailored to the island states in the Caribbean, the Pacific and the Indian Ocean. All of this is coordinated by Consumers for Dental Choice, which serves as Secretariat to the World Alliance. The ultimate goal of the Minamata Convention is the total ban on amalgam everywhere.
Progress in the USFollowing these international successes, the Chicago Declaration to End Mercury Use in the Dental Industry was created in the U.S. The declaration was signed by 50 organizations, including the Sierra Club, Clean Water Action, Greenpeace and Learning Disabilities Association of America. With these signatories onboard, the FDA finally sat up and took notice.
Efforts in Maine, Connecticut and Wisconsin RedoubleBrown expects we’ll get a ruling from the FDA by the end of 2020. If not, action within various U.S. states have redoubled. For example, the petition by Consumers for Dental Choice to the Maine dental board resulted, this year, in an official rule that all pro-mercury dentists — those still using amalgam — must provide written disclosure about the mercury in amalgam to all patients, parents or guardians. The patient must sign this disclosure, acknowledging they understand the risks before having amalgam placed in their teeth. That will undoubtedly cut back usage substantially.
Interestingly, Wisconsin actually has a law banning the sale of any product with elemental mercury aimed at children. Brown’s team is focused on applying this law to dental amalgam use, arguing to state officials that the law means use of this mercury product must end in Wisconsin children. African Region Poised to End AmalgamOn the international level, coming up in 2021 is the fourth Conference of the Parties of the Minamata Convention. The stars of the show could well be the African Region. Its 51 governments sponsored an amalgam phase-out amendment in Geneva last year, and are poised to do the same in Bali, Indonesia, next year. Brown comments:
Asian SuccessesWe’ve also seen major victories and forward movement across Asia. Indonesia has promised to end amalgam this year, but they’ve already stopped promoting it for public health. Indonesia is the fourth largest country in the world, and its version of Medicaid is far larger than that in the U.S. If they can end the use of amalgam, so can the U.S. Use of amalgam will cease in three years in the Philippines and in five years in Nepal — they serve as guides for the continent. Vietnam ended amalgam for children and for pregnant and breastfeeding women, and is working on a “road map” for amalgam’s total demise. Bangladesh ended all use of amalgam for its entire armed forces and their families, and most of its dental schools. They now teach only mercury-free dentistry and have banished the teaching of amalgam from the curriculum. Here is a great success story from the Central African nation of Cameroon, all done at the local level:
Progress in Two Nations With Massive PopulationsWhat about the two nations with a billion-plus people? Brown has made India a major priority for the World Alliance, partnering with the nation’s leading environmental group on a national campaign, and engaging a “model state” campaign in the eastern India state of Odisha. The campaign is bearing fruit. The Indian Railway, the largest employer in the world, which employs thousands of dentists for its workers, is ending amalgam use. If the world’s largest employer can end amalgam, it is less complicated for smaller employers to do the same! The World Alliance for Mercury-Free Dentistry also has allies in China.
Join the Fight to End Dental Mercury WorldwideAs you can see, significant progress is being made. We’ve come a long way in these past 10 years. With your continued support, we can end the health scourge that is dental mercury, worldwide, thereby improving the health of literally billions of people. This is the time to show your support. When you donate this week, I'm going to double your contribution, dollar for dollar, up to $150,000. We need to empower dentists who really understand health, and through that understanding provide the type of care that you and your family need and deserve. We need to eliminate this poison, and to do that we need to bring Consumers for Dental Choice across the finish line. We’re almost there.
Consumers for Dental Choice is a verified 501(c)(3) corporation, which means any donations to this campaign are tax deductible. For many of you, that means you not only can leverage your donation by my doubling any amount you give, but you also can get up to a 40% tax deduction on your donation. It's a win, win, win all around. Also, if you’re a dentist who is still using amalgam, please consider removing it from your practice immediately. Not only is it harming your patients’ health, dental amalgam is also a significant source of environmental mercury pollution. As explained by Brown:
Opt for Mercury-Free DentistryOn the home front, you can help this movement by using only mercury-free dentists. They understand the risks of mercury, refuse to expose their patients and staff to mercury vapors and protect our environment from mercury pollution. How do you find one? Here are several organizations with lists or information:
from http://articles.mercola.com/sites/articles/archive/2020/08/23/mercury-dentistry-awareness-week-2020.aspx Dr. Mercola Interviews the Experts This article is part of a weekly series in which Dr. Mercola interviews various experts on a variety of health issues. To see more expert interviews, click here. Return guest Dr. Paul Saladino is a board-certified psychiatrist and also board certified in nutrition. He wrote “The Carnivore Code,” which just came out in an updated second edition. In this interview, he discusses the impact metabolic health has on COVID-19 outcomes. He’s done a magnificent job explaining the science that supports the natural lifestyle strategies that optimize our immune systems to defeat not only COVID-19, but also most other infectious agents.
Immunometabolism Is an Important Field of MedicineWe've long known that metabolic health is crucial for robust immune function. Saladino believes immunometabolism — the connections between metabolism, metabolic health and the immune system — is easily one of the most important, if not the most important, field in emerging medicine. Saladino reviews NHANES data1 from 2009 to 2016, which reveal 87.8% of Americans are metabolically unhealthy, based on five parameters. That data is over four years old now, so the figure is clearly greater than 90% of the population today. That means virtually everyone is at risk for Type 2 diabetes and all the chronic diseases associated with insulin resistance, which run the gamut from cancer to Alzheimer’s.
Similarly, data from the U.S. Centers for Disease Control and Prevention shows that as of 2016, 39.8% of adults over the age of 20 were obese. When you include those who are overweight, that percentage skyrockets to 71%, and excess weight typically correlates with metabolic dysfunction and impaired health.
Insulin Resistance Is a Modern PlagueIndeed, while the media reports that the comorbidities include obesity, diabetes, age and being of color, they don't discuss the underlying problems, which are vitamin D deficiency and insulin resistance. As noted by Saladino:
Metabolic Age Is More Important Than Biological AgeSaladino discusses the results of a Nature Medicine study2 published in 2019, which looked at immune age and metabolic age using high-dimensional longitudinal monitoring:
So, the overarching principle is that it's not your biological age that matters so much, but rather it’s your immune and metabolic age. The good news is those are more malleable than we are led to believe. From that perspective, we can address COVID-19 in completely different ways.
CytokinesCytokines are small proteins secreted by cells in your innate and adaptive immune systems. They serve to regulate diverse functions in your immune response. Cytokines are released by cells into your circulation or directly into your tissues. 
The cytokines locate target immune cells and interact with receptors on the target immune cells by binding to them. The interaction triggers or stimulates specific responses by the target cells. In response to bacterial and viral infections such as COVID-19, your innate immune system generates both proinflammatory and anti-inflammatory cytokines.3 The inflammatory response plays a crucial role in the clinical manifestations of COVID-19. SARS-CoV-2 triggers an immune response against the virus, which, if uncontrolled, may result in lung damage, functional impairment, and reduced lung capacity.4,5,6,7 The SARS-CoV-2 viral infection-related inflammation and the subsequent cytokine storm in severe cases plays a crucial role in patient survival.8 The extensive and uncontrolled release of proinflammatory cytokines is termed the cytokine storm. Clinically, the cytokine storm commonly presents as systemic inflammation and multiple organ failure.9 Immunologic Tolerance Rises as Insulin Resistance FallsOne scientific article10 that speaks to this is “Association of Blood Glucose Control and Outcomes in Patients With COVID-19 and Pre-Existing Type 2 Diabetes,” published in Cell Metabolism, June 2, 2020. What it found was that when blood sugar is well-controlled and there's less glycemic variability, people do better when contracting COVID-19. When they have high levels of glycemic variability, which is indicative of insulin resistance, they fare much worse. “So there's really no question at this point that glycemic variability, overall metabolic status, overall metabolic health are critical,” Saladino says. The common mistake here is that you don’t want to get that control back using drugs. Your best bet is to get it back using natural lifestyle strategies. Another paper11 that demonstrates the impact of insulin resistance on COVID-19 was published in Cardiovascular Diabetology, May 11, 2020. It found you can use the triglyceride to glucose index (TyG index) as a gauge to predict the severity and mortality of COVID-19.
Low LDL Associated With Greater COVID-19 SeverityInterestingly, Saladino cites research showing that low levels of LDL cholesterol are associated with greater COVID-19 severity. LDL and total cholesterol levels were significantly lower in COVID-19 patients as compared to healthy subjects. “To me, this is a really interesting [finding] in two ways,” Saladino says, adding:
Top Strategies to Improve Your Metabolic HealthConsidering the fact that your metabolic health determines your COVID-19 risk, it would be a sound idea to implement strategies that will improve your metabolic flexibility and insulin sensitivity. Saladino’s top recommendations for achieving that include: 1. Eliminate processed carbohydrates, sugars, grains and vegetable oils -- “I think that from a food perspective, those are the key evils that are really wreaking havoc on our metabolism,” he says. The worst culprit of them all is probably vegetable oils. “Polyunsaturated vegetable oils are highly oxidizable and very metabolically damaging. So, start with them,” Saladino says. For more information about this, see “New Study Tells Why Chicken Is Killing You and Saturated Fat Is Your Friend,” which features Saladino’s interview with science journalist and author, Nina Teicholz. Saladino also reviews the mechanisms by which vegetable oils wreck health in greater detail in this interview, so be sure to listen to it in its entirety, or read through the transcript. 2. Eat animal foods -- As noted in the paper,12 “Immune Function and Micronutrient Requirements Change Over the Life Course,” published in the journal Nutrients, nutrient deficiencies that can compromise immune function include vitamins, A, C, D, E, B2, B6, B12, folate, iron, selenium and zinc. These vitamins are primarily found in animal foods, which is why shunning animal foods tends to lead to nutrient deficiencies. Even folate is found in organ meats in highly bioavailable form. “If you want to have a robust immune system, you want to be metabolically healthy. You don't want to be insulin-resistant and you need to have nutrient adequacy in your diets,” Saladino says. “How do you get nutrient adequacy? You get these micronutrients from bioavailable sources in organ meats and in the muscle meat of animals.” If you cannot stomach the idea of organ meats, consider using a desiccated organs supplement, such as those Saladino sells.13 3. Time-restricted eating -- Compressing the window of time in which you eat down to six to eight hours a day, eating your last meal at least three hours before bedtime, is another very powerful strategy to improve your insulin sensitivity. Eating a Varied, Real Food Diet Is KeyIn short, eating real food, in a time-restricted window, is your surest bet to beat insulin resistance. Also remember to give some consideration to your macronutrient ratios. As explained by Saladino, while a low-fat, high-carb diet may reduce your insulin resistance, you’re at high risk for nutrient deficiencies in the long term, as so many of the most bioavailable vitamins and minerals are found in animal-based fats.
Low Glutathione May Increase COVID-19 SeveritySaladino also cites a recent hypothesis highlighting the potential role of glutathione in COVID-19. The paper,14 “Endogenous Deficiency of Glutathione as the Most Likely Cause of Serious Manifestations of Death From Novel Coronavirus Infection (COVID-19): A Hypotheses Based on Literature Data and Own Observations,” is written by a Russian medical doctor and Ph.D. What he found was that the reactive-oxygen-species-to-glutathione ratio was able to predict the severity of COVID-19 and the patient’s outcome. When the patient had a low ROS-to-glutathione ratio, the patient had a very mild case. The fever disappeared on the fourth day without any treatment whatsoever. When the ROS-to-glutathione ratio was high, the patient developed air hunger on the fourth day, experienced significant fever, hoarseness, myalgia and fatigue persisting for 13 days. A patient with even higher ROS and lower reduced glutathione had critical disease requiring hospitalization for COVID-19-related pneumonia. According to the author:15
Glutathione, Zinc and SeleniumAs noted by Saladino, these findings also tie into the issue of zinc and its importance for proper immune function, as zinc helps mitigate the oxidative stress reaction. The question is, why do these people have such low glutathione in the first place? Saladino believes it’s probably due to underlying nutritional deficiencies such as glycine deficiency, or oxidative stress caused by smoking, heavy metal toxicity, EMF exposure, eating lots of processed vegetable oils or insulin resistance. Any of these could cause low glutathione. To improve your glutathione, you need zinc, and zinc in combination with hydroxychloroquine (a zinc ionophore or zinc transporter) has been shown effective in the treatment of COVID-19. N-acetyl cysteine (NAC), meanwhile, is a precursor of glutathione, and may protect against coagulation problems associated with COVID-19, as it counteracts hypercoagulation and breaks down blood clots. Selenium is also important, as some of the enzymes involved in glutathione production are selenium-dependent. Saladino cites research showing an association between regional selenium status and the severity of COVID-19 outcome cases in China. The lower the amount of selenium in the hair, the lower the cure rate was.
One of the best ways to increase glutathione, though, is molecular hydrogen. It is my absolute favorite as it does so selectively and will not increase glutathione unnecessarily if you don’t need it. You can view Tyler LeBaron’s excellent lecture on the details of how it does this in “How Molecular Hydrogen Can Help Your Immune System.” More InformationWe cover a lot of ground in this interview, far more than has been summarized here, so for more details, be sure to listen to the interview. Saladino is a wellspring of well-researched information. We also review:
To learn more, be sure to visit his website, CarnivoreMD.com, and pick up a copy of “The Carnivore Code,” now in its updated second edition. He also has a great podcast called “Fundamental Health.” On the social media platforms, you can find him by searching for @carnivoreMD.
from http://articles.mercola.com/sites/articles/archive/2020/08/23/metabolic-health-impact-on-covid-19-severity.aspx |
Nia Pure NatureThe Provider of premium Quality Health Products To Live Better Lives Archives
March 2022
Categories |
 RSS Feed
RSS Feed
