|
Once the social, economic and medical implications of COVID-19 had a hold on society, all eyes turned from nearly every other environmental and health-related concern to focus solely on the controversies and debates about how to treat and contain the virus and what to do about a vaccine. These are just some of the economic, political and social challenges people are facing: • The initial panic resulted in the purchase of $3 billion worth of ventilators, 79,295 of which The Washington Post reports are sitting unused.1 • The question of whether or not to wear a mask has become one of the most hotly contested debates, despite research over the past decade demonstrating cloth masks are ineffective against viruses.2 • Hiding under the guise of “biodefense” and “biomedicine,” a network of virologists, military scientists and biotech entrepreneurs are weaponizing microorganisms and growing an arsenal of Frankenstein pathogens. But as investigative reporter and bioweapons expert Sam Husseini writes, gain-of-function/biowarfare scientists in labs such as Wuhan, China, and Fort Detrick, Maryland, have been accused of deliberately and recklessly conducting nefarious types of research.3 • As part of Operation Warp Speed, Pfizer struck a $1.95 billion deal to provide the U.S. with 100 million doses of its COVID-19 vaccine to give the U.S. public for “free,” with an option for 500 million more.4 • As some people are considering whether they will submit to yet another vaccine, Yale University is conducting trials to determine the type of message that will maximize the number of people who will accept and use the vaccine.5 In other words, they are testing messages that will trigger an emotional response to raise the potential that you will say yes. This is a blatant and highly sophisticated form of salesmanship. The types of messages under investigation include those that address your personal freedom, self-interest, economic benefit and guilt. The core message throughout this pandemic should have been how to protect your health and reduce the risk of severe disease. But, it hasn’t been. Instead, minor wars are being waged over financial decisions that may have little to do with you. Sunlight Negatively Correlated With Positive TestingHuman coronaviruses are named for the appearance of spikes on the surface. There are four main subgroups, the first of which was identified in the mid-1960s. To date, the CDC has identified seven types of coronavirus that can infect humans, including MERS, SARS and SARS-CoV-2.6 Without the fanfare that has accompanied the proposed release of remdesivir, an antiviral medication costing $3,120 per dose to treat COVID-19,7 recently published data again revealed the simple and cost-free act of sensible sun exposure for fighting SARS-CoV-2 and four other human coronaviruses.8 The research team began with the knowledge that RNA viruses, such as human coronaviruses, are sensitive to ultraviolet radiation from the sun and that the “incidence and mortality of coronavirus disease 2019 (COVID-19) are considered to be correlated with vitamin D levels.” Using these two points as a foundation, they sought to analyze the correlation between five types of human coronavirus and how much sunlight was needed for a negative test. Measurements were taken from April 17, 2020, to July 10, 2020, during which time the researchers found there was a significant negative correlation in four viruses with the amount of sunlight and a percent positive test. The U.S. has four census regions, which the researchers used to categorize the findings. Census region No.1 includes the Northeast states bordered in the south by Pennsylvania. Census region No. 2 includes North Central states bordered on the south by Illinois, Indiana, Ohio, Missouri and Kansas. Census No. 3 includes the Southern states bordered on the west by Texas and on the east by Florida’s Atlantic coast. Census region No. 4 is the West Coast, boarded on the east by Montana, Wyoming, Colorado and New Mexico. Data indicate census regions 1 and 2 had a significant negative correlation with sunlight exposure (meaning sunlight reduced coronavirus infection), while regions 3 and 4 had a minimal positive correlation that was not statistically significant. The difference in these two areas may be explained by the significant heat during those months, driving people indoors to air conditioning. Vitamin D Deficiency at Pandemic LevelsAs more research demonstrates the effectiveness vitamin D has against infectious diseases and COVID-19, it's important to note that vitamin D deficiency across the world is also at a pandemic level. Deficiencies have been found in countries in the Southern Hemisphere where it was assumed there was enough exposure to UV radiation to prevent a vitamin D deficiency.9 However, a variety of factors likely influence this difference. For instance, the authors of one literature review found that women from the Middle East were particularly low in vitamin D.10 However, since many people in Middle Eastern countries practice Islam and the women do not go outside unless they are fully covered, the skin's ability to produce vitamin D with exposure to the sun is inhibited.11 Another study involved the use of an international Vitamin D Standardization Program led by the National Institutes of Health to evaluate 14 population studies.12 The data showed that regardless of age, ethnicity or latitude, 13% of the 55,844 Europeans who were tested had serum vitamin D levels less than 12 ng/mL (30 nmol/L). When an alternate level of deficiency was used, less than 20ng/mL (50 nmol/L), the prevalence was even higher at 40.4%. Additionally, when the group was subdivided by ethnicity, the data showed people with dark skin had a much higher level of deficiency than white populations, at rates of up to 71 times higher. Sunscreen Advice Counter to Lifesaving Vitamin DRemarkably, as the importance of vitamin D becomes more widely recognized, some doctors are continuing to advise against sensible sun exposure, vitamin D supplementation or both. For example, Dr. Pieter Cohen is an internal medicine physician at Cambridge Health Alliance in Massachusetts who has not recognized the importance of vitamin D at this time. In an interview with Today, Cohen told the reporter he strongly discourages people from even getting a vitamin D test, and went on to say:13
As sensible sun exposure and vitamin D supplementation are relatively innocuous with little to no side effects when done appropriately, it seems rather peculiar to recommend people should not even be tested or take a supplement for the potential benefit they may receive. The advice to use sunscreen while getting “incidental” exposure is also medically incorrect, since sunscreen filters out the ultraviolet rays that stimulate vitamin D production in your skin. In order for sensible sun exposure to work, your skin must be unprotected, and you should be sure you don't get sunburned. Stay out until your skin turns the lightest shade of pink and then cover with long sleeves and pants. Positive Tests and Deaths Declined Over the SummerMany respiratory illnesses decline over the summer. While it’s still possible to get a cold or flu, it’s less likely during the summer months. Since mid-July, indicators from the CDC show COVID-like illnesses and positive tests have declined in the U.S.14 The CDC also gathers data to tally the number of deaths from COVID-19 and pneumonia while excluding flu. The first death in this category was recorded February 22, 2020.15 The number peaked the week of April 18, 2020, at 7,292 deaths. By end of June the number had dropped significantly to 1,530. However, as a new report from the CDC reveals, 94% of the deaths attributed to COVID-19 happened in people who had other significant health conditions and contributing causes.16 For only 6% of the deaths, COVID-19 was the single cause on the death certificate. To make this comparison, it's the difference between an individual dying FROM COVID-19 versus WITH COVID-19, since for many with a positive test they are asymptomatic and therefore do not qualify as a “case” of COVID-19 but, rather, as a positive test. Some of the top contributing conditions were cardiac arrest, heart or renal failure, vascular or unspecified dementia, and influenza and pneumonia.17 In addition to rising vitamin D levels during the summer months, there are other factors that influence the transmission of infectious diseases and slow the spread. For instance, influenza is affected by both temperature and humidity.18 In one study conducted in New South Wales, Australia, researchers found a similar connection between humidity and COVID-19. A 1% decrease in humidity was predicted to increase the number of cases by 6.11%.19 In a separate study, the addition of a humidifier in the bedroom demonstrated a decrease in the survival of influenza virus, by 17.5% to 31.6%.20 During the cold winter months, people also spend more time indoors, in enclosed spaces with less ventilation. The same can be said during the heat of the summer when people seek relief indoors with air conditioning. During the fall and winter months, school is usually in session, which has been associated with a higher transmission of respiratory viruses. Marc Lipsitch, professor of epidemiology and director of the Center for Communicable Disease Dynamics at the Harvard T.H. Chan School of Public Health also notes:21
Combine These Strategies With Raising Your Vitamin D LevelVitamin D optimization is a powerful and beneficial strategy to protect your health. In my free report on vitamin D I've developed a resource you can use to share and help educate others. The only way you’ll know your vitamin D level is to test it. GrassrootsHealth has a home test kit that is simple to use and provides you with results at home.22 You’ll find a calculator at GrassrootsHealth.net that uses your current weight, serum level and daily supplement intake to estimate how much vitamin D3 you need to reach your desired vitamin D level.23 Yet, while crucial, it’s not the only thing available to help protect your health. It’s particularly important to become metabolically flexible to help reduce the severity of a COVID-19 infection. The single most important step to attaining and maintaining metabolic flexibility is to reduce the number of hours during the day in which you eat. When you do this, you decrease insulin resistance. In my book Fat for Fuel I discuss how to become metabolically flexible, including using intermittent fasting and cyclical nutritional ketosis. The use of molecular hydrogen is another strategy, as it's a powerful antioxidant and an anti-inflammatory agent. Using quercetin with zinc can further lower your risk. Quercetin acts as a zinc ionophore24 and has its own antiviral effects.25 One of the best treatments today is the MATH+ Protocol, first developed by the Front Line Covid-19 Critical Care Alliance.26 It's designed to be used when someone is hospitalized and needs supplemental oxygen. You'll find further information about each of these strategies in "How to Fix the COVID-19 Crisis in 30 Days." from http://articles.mercola.com/sites/articles/archive/2020/09/26/sunlight-makes-coronavirus-tests-turn-negative.aspx
0 Comments
The idea that electromagnetic fields (EMFs) can impact your brain function is not new, but a recently launched investigation by the U.S. Defense Advanced Research Projects Agency (DARPA) really highlights the reality of such concerns. The program,1 “Impact of Electro-Magnetics on Aircrew Neurology,” or ICEMAN, seeks to determine whether EMFs inside the cockpit may be causing pilots to crash. DARPA is currently accepting proposals and have allocated a budget of up to $225,000 for the research. According to DARPA, the objective of the ICEMAN program is to “Determine if the current air combat cockpit environment impacts cognitive performance and/or physiological sensor performance; quantify the effects; and demonstrate potential mitigation strategies.”2 Is Pilot EMF Exposure Causing Aviation Crashes?As noted by DARPA,3 fighter pilots operate in a very high-EMF environment these days, and it’s possible those EMFs may be causing pilots to become disoriented and confused, leading to plane crashes.4 Over the past few years, there’s been a rather extraordinary string of military jet and helicopter crashes. Back in 2018, following a series of three aviation crashes that killed five service members over the course of two days, the director of the Pentagon’s joint staff tried to downplay the trend, rejecting questions suggesting military aviation was in a crisis, stating:5
In 2017, 37 service members died in noncombat crashes. By April 2018, there had already been five noncombat aviation crashes that year, killing nine service members. In December 2018, six Marines died during a refueling crash off the coast of Japan.6 The pilot, who died, was accused of losing situational awareness and causing the crash due to atypical maneuvering. As reported7 by Fox News in April 2018, there were also several additional crashes and emergency landings that year that did not result in fatalities. Several noncombat air crashes also occurred in 20198,9 and 2020.10,11,12,13,14,15 Canada has also reported unusual military aviation crashes.16 The ICEMAN ProgramAccording to DARPA:17
The ICEMAN project aims to determine “what effect, if any, the cockpit RF/EM environment may have on physiological sensor function and efficacy” by measuring and manipulating ambient EM and RF fields inside the cockpit to determine their effects on “brain activity, physiology, behavioral responses and physiological sensing systems.” Lastly, the program seeks to determine if and how any negative effects on neurology and sense function might be effectively mitigated. All of this is a rather extraordinary admission that EMFs have neurological and physiological effects — a claim made by many scientists involved in EMF research that has been roundly dismissed as unsubstantiated and false by the wireless industry and regulators. Yet here is DARPA, admitting research has demonstrated that RF waves impact brainwaves and behavior. Mechanisms of HarmMartin Pall, Ph.D., Professor Emeritus of biochemistry and basic medical sciences at Washington State University, has published research18,19,20,21 showing one of the primary mechanisms by which EMFs harm your biology is through the creation of peroxynitrites, which are potent sources of oxidant stress and secondary free radicals. Low-frequency microwave radiation activates the voltage-gated calcium channels (VGCCs) in the outer membrane of your cells, causing them to open, thus allowing an abnormal influx of calcium ions. This activates nitric oxide, which combines with superoxide to form peroxynitrite.22 These potent reactive nitrogen species are associated with an increased level of systemic inflammation and mitochondrial dysfunction, and are thought to be a root cause for many of today's chronic diseases. One of its most significant downsides of peroxynitrite is that it damages your DNA. While your body has the capacity to repair that damage through a family of enzymes collectively known as poly ADP ribose polymerases (PARP), PARP require NAD+ for fuel, and when they run out of NAD+ they stop repairing your DNA, which can lead to premature cell death. EMFs also damage your health in other ways. For example, the enzyme ATP synthase — which passes currents of protons into the mitochondrial intermembrane space, similar to current passing through a wire — powers the generation energy of the creation of ATP from ADP, using this flow of protons. Magnetic fields can change the transparency of the flow of protons to the mitochondrial intermembrane space, thereby reducing the current. As a result, you get less ATP, which can have system wide consequences, from promoting chronic disease and infertility to lowering intelligence. How EMFs Cause Neuropsychiatric ProblemsIn a 2016 paper,23 Pall describes how EMFs can trigger neuropsychiatric problems specifically. As mentioned, EMFs trigger the opening of VGCCs, thereby causing a chemical cascade resulting in the production of harmful peroxynitrites. Your brain and nervous system have a particularly high density of VGCCs, which is why these areas are particularly prone to the impacts of EMF. VGCC activation also triggers excessive neurotransmitter and neuroendocrine release.24 Considering the neurological effects demonstrated in many different studies over the course of decades, it seems entirely reasonable to suspect some pilots are being cognitively impaired by EMFs inside the cockpit, some to the point of losing control of their aircraft. As explained in Pall’s paper:25
Six Common Types of EMF StressVirtually everyone needs to consider EMF remediation these days. At bare minimum, everyone needs a low EMF environment during sleep, in order to prevent accelerated aging and everything that goes with it. Your body rejuvenates and detoxes during sleep and if your body is bombarded with EMFs all night long, it won’t be able to effectively perform those crucial cleanout and regenerative functions. Sleeping in an EMF-free environment can go a long way toward avoiding electrosensitivity, which by the way tends to come on very rapidly, in many cases seemingly “overnight.” Common symptoms of electromagnetic hypersensitivity include ringing in the ears, distress when exposed to fluorescent lights, a feeling of burning or prickling in the skin, headache, heart palpitations and inexplicable anxiety, for example. Once you’re electrosensitive, additional and more extensive remediation strategies may become necessary. While not as saturated as the cockpit of a fighter plane, the average home today is bathing in EMFs from a wide range of electronics and wireless gadgets. Six primary sources of EMF stress that can impact your health are:
We’ve Been ‘EMF*D’Over the past decade, I’ve written many articles discussing the evidence of biological harm from nonionizing EMF radiation, which I believe is one of the greatest challenges to public health facing us today. For a refresher, see my previous article, “Reduce EMF Exposure.” These challenges will only get worse now that 5G is being rolled out across the globe. For a recap on the additional hazards brought on by 5G, see “5G Apocalypse: The Extinction Event,” which features a documentary by the same name, or “Scientific American Warns: 5G Is Unsafe.” My book “EMF*D” is an attempt to inform you about the hidden harms of EMF and what you need to do to protect yourself and those you love. I also reveal the reasons why you’ve been left in the dark about this serious health threat. In it, I review:
The tragedy is that 5G isn’t even necessary. As discussed in “War Against 5G Heats Up,” the American public has already paid for the implementation of fiber optic cables across the country, which would be far safer and just as fast as 5G. State utilities stole that money and illegally redirected it toward wireless infrastructure instead. from http://articles.mercola.com/sites/articles/archive/2020/09/25/emf-level-in-aircraft-cockpit.aspx The number of people who struggle to attain and maintain a healthy weight continues to grow each year. Data from the National Health and Nutrition Examination Survey 2017-2018 showed that 42.4% of adults in the U.S. were obese.1 The prevalence of severe obesity was 9.2%, and it was higher in women than in men. The weight loss market also continues to grow, as it expanded by 4.1% in 2018 and is expected to grow 2.6% each year through 2023.2 Yet, the growth in the market is not in prescription drugs, diet soda or weight loss franchises. Instead, meal replacement shakes and bars as well as weight loss surgeries appear to be holding steady and growing. Dieters are also searching for more “clean” options, free of GMOs and artificial additives. This has forced companies supplying diet dinners and other premade foods to reformulate their offerings. While the focus on weight loss is often on how to look better or meet a certain standard, weight management should be about how to live free of disease. Carrying excess weight is linked to heart disease, Type 2 diabetes, stroke, high blood pressure and certain cancers.3 In addition to these long-term health concerns, it is also associated with an increased risk of certain infectious diseases, such as COVID-19. Can You Eat Less and Live Longer?People have been searching for the “fountain of youth” for centuries. Yet, the goal isn’t just to live longer but to live longer while free of disease and illness. Scientists call this your health span — the number of years you live without disease. Researchers have been studying two ways to achieve eating less. The first is called calorie restriction, in which the number of calories is limited each day without malnourishing or depriving your body of essential nutrients.4 In the second method, fasting, a person eliminates or severely restricts calories during the day, week or month. Based on the results from a study involving animals, one of the ways calorie restriction has promoted a longer health span is by decreasing the core body temperature.5 Researchers sought to evaluate the effect that a drop in core body temperature has on the ability of calorie restriction to improve one’s health span. They compared the responses of mice on a calorie-restricted diet that were housed in a temperature-controlled room. In this study, the focus was on temperature as a driving factor. One group of mice was kept in a room with a temperature of 71.6 degrees Fahrenheit (F) and the other group at 86 degrees F. The warmer room offered what scientists call thermoneutrality. This is a balance between the temperature of the organism and the environment so that the regulation of internal temperature remains inactive. In each room, half the mice were given as much food as they wanted, and the other half had their diet restricted by half. Throughout the course of the study, the metabolic activity in the hypothalamus and blood plasma were measured. The data revealed that the mice in the cooler room had greater changes in life-extending factors. There were fewer changes in the group of mice living in the warmer room. Science Is Seeking a Pharmaceutical ‘Easy Button’Further examination of the results showed that the metabolic effects were linked to nitric oxide and leucine enkephalin. These were produced in higher amounts in the animals in the cooler room. Leucine enkephalin is an endogenous opioid neurotransmitter6 that scientists believe directly controls core body temperature.7 Bruno Conti, from the department of molecular medicine at Scripps Research, was one scientist from the study. He spoke with a reporter from Inverse about the results and the phenomenon of dropping core temperatures that has been seen in calorie restriction in other animal studies, saying:8
As the reporter from Inverse writes, “Years down the line, researchers predict people may be able to derive some of calorie restriction's positive benefits — without actually reducing what they eat.”9 Yet, as with all pharmaceutical interventions, there will likely be side effects and adverse events that a person will not experience with intermittent fasting. Evidence Shows Health Benefits in Humans and AnimalsFor a further look into how calorie restriction affects human health, the National Institute on Aging, the National Institute on Diabetes and Digestive and Kidney Diseases and Duke University School of Medicine undertook a clinical trial called Comprehensive Assessment of Long-term Effects of Reducing Intake of Energy (CALERIE).10 The study engaged 218 individuals who were of normal weight or who were moderately overweight. Each person was randomly assigned to one of two groups.11 Participants in the experimental group were asked to eat a calorie-restricted diet for two years consisting of 25% fewer calories than they normally ate before the study. The control group ate their regular diet. At the end of two years they found that members of the experimental group were able to reduce their calories by 12%. They lost 10% of their body weight and sustained much of that loss. The intervention group also lowered their blood pressure and cholesterol measurements, both of which are risk factors “for age-related diseases such as diabetes, heart disease, and stroke.”12 Additionally, those eating a calorie-restricted diet showed no adverse effects in their sleep patterns, sexual function, quality of life or mood. While the data showed some slight decline in bone density, lean body mass and aerobic capacity, they were not more than would generally be expected based on the weight loss the individuals experienced. In 2012, the National Institute on Aging (NIA)13 published the results of a study whose premise was similar to that of a 2009 study conducted by leaders at the University of Wisconsin.14 Each set of scientists set out to explore the idea that a calorie-restricted diet in rhesus monkeys could affect life span and health span. The results from the two studies were different, so in 2017 the researchers teamed up to resolve the discrepancies by comparing data.15 The group from the University of Wisconsin fed monkeys a calorie-restricted diet with 30% fewer calories than the control group. The monkeys survived an above-average number of years as compared to other rhesus monkeys in captivity. Although the NIA study did not find a significant effect on aging, both groups found fewer age-related health conditions as compared to the control groups.16 When the data were compared, researchers found significant differences in the types of diet, the timing of feedings and the initial age and genetics of the groups. Scientific American reports that the researchers described one monkey that was started on the restricted diet at a late middle age of 16 years.17 At the end of the study he was 43 years, which is a record for this species and equal to a person living 130 years. Calorie Restriction Sets Off HormesisThe term hormesis refers to a dose-response relationship between a stimulus and a biological effect. There are significant health benefits from hormesis. Siim Land is a socio-cultural anthropologist, entrepreneur and high performance coach who wrote "Metabolic Autophagy: Practice Intermittent Fasting and Resistance Training to Build Muscle and Promote Longevity (Metabolic Autophagy Diet Book 1)."18 In his book Land defines hormesis, which can be summarized as, “what doesn't kill you is going to make you stronger.” In some cases, public health officials have used this notion to justify the release of low-level toxic exposure claiming it would ultimately be beneficial.19 The concept describes the fundamental need to adapt to various types of stimuli to enhance survival. It also produces effects that are similar to autophagy since it is stimulated by like pathways. For instance, intermittent fasting or calorie restriction is a stressor that activates hormesis. As Land describes in my interview with him, others are high-intensity exercise and exposure to cold or heat.20
Cell biologist Rhonda Patrick, Ph.D., has described how the adaptation to stress also effectively boosts mitochondrial biogenesis. These short bouts of stress activate response pathways that are encoded in your genes.21 As I have discussed in the past, optimizing mitochondrial function is at the heart of optimal health and extremely important in disease prevention. Your mitochondria are the energy storehouses in most cells. They perform interconnected functions that contribute to stress responses, such as autophagy and apoptosis.22 They form an interconnected network throughout the body that influence physiology and affect communication between the tissues and the cells. They have emerged as crucial in the development of diseases, including metabolic disorders and neurodegenerative disease. This means you can activate hormesis and mitochondrial biogenesis using intermittent fasting to achieve your goal, essentially helping to lengthen health span. Another type of environmental stress that activates these pathways is exposure to heat and cold. In a past article, “The Surprising Health Benefits of Extreme Hot and Cold Temperatures,” I discuss these concepts with Patrick and their relationship to heart and brain health as well as athletic performance. Make Intermittent Fasting and Cyclical Ketosis Work for YouIntermittent fasting contributes to the realization of several health benefits, including longevity and health span. This is an eating pattern that seeks to mimic some of the habits of our ancestors, who had to survive when food was not available around the clock. Intermittent fasting restores your body to a more natural state. It's become clear that a continuous supply of calories does not provide your body with the optimal environment for maintaining health. Also important to life span and health span is making the shift from carbohydrate burning to fat burning by combining intermittent fasting with a cyclical ketogenic diet. I discuss many of the strategies for doing so in, "Why Intermittent Fasting Is More Effective Combined With Ketogenic Diet." There are many benefits to intermittent fasting, including a newly discovered function of raising the production of antioxidants and age-related metabolites.23 These metabolites have an antiaging effect on the body and they stimulate metabolism. There are some points to consider as you change your eating habits, however. For instance, intermittent fasting does not have to be a form of calorie restriction. Instead, you restrict the number of hours you're eating during the day. It's also important to remember that any sugar cravings will be temporary and they’ll slowly go away as your body begins to burn fat as its primary fuel. However, as healthy as intermittent fasting is, you shouldn’t use it if your diet is filled with processed foods. Intermittent fasting is not a panacea against ill-health and excess weight, and as with all health choices, must be made with consideration for your total approach to vitality and well-being. from http://articles.mercola.com/sites/articles/archive/2020/09/25/eating-less-positive-effects-on-metabolism.aspx Over the last decade, there has been a significant increase in vaccine related legislation that impacts every person. More vaccines have been mandated for children in school and daycare and adults in the workplace, vaccine exemption rights have been restricted or removed, emergency powers have been expanded, vaccine tracking and enforcement and vaccine exemption rate disclosure programs threaten choices and health outcomes, and parental and informed consent rights have been weakened or removed all together. This has all happened under the backdrop of unprecedented censorship of information questioning the safety, efficacy or necessity of the dozens of vaccines being mandated for use and the hundreds of vaccines in development. Public shaming, marginalization and the bullying of those who don’t agree with accepting every single dose of every federally recommended and state mandated vaccine has become not only commonplace but socially sanctioned by those promoting “no exceptions” vaccine policies and laws. In addition, with the declaration of a COVID-19 pandemic in March 2020, plans to roll out a national vaccination program loom on the horizon. If the COVID-19 vaccine becomes state mandated, it has the potential to alter life in America in ways we never thought could be possible. Citizen involvement in the legislative process to protect the human right to exercise informed consent to vaccination increased to unprecedented levels in 2020. In many cases, it matched and overcame the relentless attack by mandatory vaccination proponents on the ability of individuals to decline vaccination. Highest Number of Vaccine-Related Bills in NVIC’s HistoryIn this 2020 Annual Report on U.S. State Vaccine Legislation, the non-profit educational charity National Vaccine Information Center (NVIC) reports that during the 2020 legislative session, NVIC analyzed, tracked and issued positions on an unrivaled 232 vaccine related bills in 39 states and the District of Columbia through the NVIC Advocacy Portal. This was the highest number of bills in the history of NVIC’s advocacy program, despite many shortened state legislative sessions due to COVID-19 social distancing restrictions. 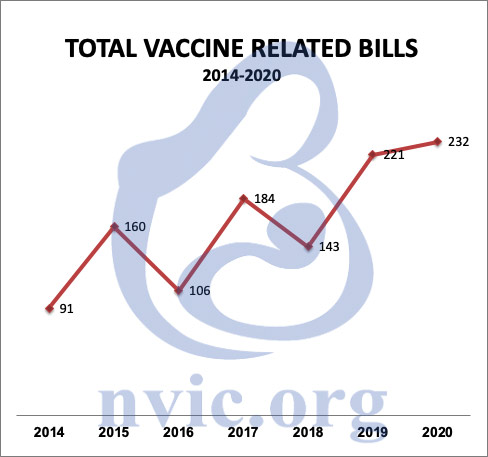
Working to prevent vaccine injuries and deaths through public education since 1982, NVIC is the largest and oldest U.S. consumer-led non-profit organization disseminating information about diseases, vaccines and informed consent to vaccination. NVIC provides well-referenced, accurate information to the public about vaccine science, policy and law but does not make vaccine use recommendations. In 2010, NVIC launched the NVIC Advocacy Portal (NVICAP), a free online vaccine choice advocacy network, for the purpose of securing and defending informed consent protections in vaccine policies and laws. Over the last decade, the NVIC Advocacy Program has analyzed, tracked and issued positions on well over 1000 vaccine related bills and has worked alongside and shares legislative information with many health freedom groups that support NVIC’s almost four-decade call for the protection of vaccine informed consent rights in America. The NVIC Advocacy Portal team, including key NVIC Advocacy directors in many states, works with families and enlightened health care professionals to educate legislators and protect vaccine informed consent rights. NVIC issues action alerts and sends them through email, posts them online and shares them through social media and our text alert program. 
At the time this report was prepared, vaccine-related bills are still pending in California, District of Columbia, Illinois, Massachusetts, Michigan, New Jersey, New York, Ohio, Pennsylvania, Virginia, Vermont, and Wisconsin. Action to support the good vaccine-related bills and oppose bad bills is still needed. Bills referenced in this report are published on the NVIC Advocacy Portal and registered users can obtain a more detailed bill analysis, including current status, NVIC’s position on the bill, and recommended action. Highlights From 2020There were significant positive take away points from the outcome of the 2020 legislative session:
The remaining vaccine-related bills for the 2020 session are broken out and described below by category. 2020 Bill Analysis by CategoryThe four main areas that NVIC focuses on when tracking proposed bills are:
Some bills may be included in multiple categories. For example, a proposed bill attempting to mandate a vaccine may also have a requirement for vaccine tracking so it would be counted in both categories but only counted once in the total bill count. The NVIC Advocacy team provides referenced, accurate vaccine information and talking points for NVICAP users to background legislators. Some of the position statements NVIC posted on the Advocacy Portal in 2020 were listed as bills to “watch.” This is done because our analysis indicated that either the bill was well intentioned but contained some problems needing amending before we could support it or the bill contained sections that were highly vulnerable to amendments that could conflict with NVIC’s mission. The breakout and analysis of bills in these different categories identifies trends across the states and serves as a guide if you want to become active by joining the NVIC Advocacy Portal and educating your state legislators and community in 2021 about why it is so important to protect vaccine informed consent rights. Vaccine Exemptions and Informed Consent (138 Bills)In a positive turnaround from previous sessions, out of the 138 vaccine-related bills filed in state legislatures in 2020 having components affecting vaccine exemptions and informed consent rights, NVIC opposed 56 of the proposed bills, but supported 78 and “watched” four. This is the first session where NVIC has supported more exemption and informed consent bills than opposed. The mainstream media tended to hype the bills attacking exemptions so much that it may come as a surprise that there were more bills to expand exemptions and informed consent rights than there were to eliminate or restrict those rights. This can be directly credited to positive action taken by forward thinking state legislators, who were given fact-based information about vaccines, exemptions, and diseases by concerned citizens who took the time to make one-on-one personal contact with their elected representatives. Eliminating or Restricting Vaccine ExemptionsThere was a noticeable drop in bills filed in 2020 to either remove or restrict exemptions: 23 in 2020 versus 40 in 2019. There were 13 bills in 10 states (Connecticut, Florida, Iowa, Illinois, Massachusetts, New Jersey, Pennsylvania, Vermont, Washington and Wisconsin) that were filed to eliminate vaccine exemptions. None passed. Notable in these defeats was Connecticut HB 5044 attempting to remove the religious exemption, which broke all records for online testimony that gripped the country overnight and lasted over 21 hours into the next morning. This bill did not pass. Florida SB 64 to remove the religious exemption was filed by Senator Lauren Book in 2019 before the 2020 legislative session even started. This prompted families around the state to fight back by attending local pre-session delegation meetings asking for the bill’s defeat. Health Freedom Florida hosted a rally featuring presentations by NVIC and Children’s Health Defense the first week of session to educate citizens about the bill. This proactive strategy was effective. SB 64 failed to pass and did not even get a hearing. New Jersey’s religious exemption removal bills (A969/S902) drew more in person protests than any vaccine bill had done before with many thousands showing up to oppose the exemption removal. Legislators inside the capitol building could hear protesting parents chanting for hours outside. This bill came the closest to passing of all the exemption removal bills. The strong showing by New Jersey families helped provide support to the brave legislators opposing this bill. Out of 10 bills filed across eight states (Colorado, Florida, Massachusetts, New Jersey, New York, Oklahoma, Pennsylvania and Vermont) to restrict vaccine exemptions, only one passed. Colorado SB 163 requires a vaccine provider signature or the completion of an online re-education module for religious or conscientious exemptions. Bills pending to remove or restrict vaccine exemptions that deserve continued strong opposition are still active in Illinois, Massachusetts, New Jersey, New York, Pennsylvania, and Vermont. These bills need to continue to be opposed. It is critical that vaccine choice advocates in every state register for and regularly check in to the NVIC Advocacy Portal. The most important thing you can do if you care about this issue is to establish relationships with and educate your legislators now and into next year so you can be ready to counter bills that will restrict or eliminate exemptions and get good bills filed to protect and expand vaccine exemptions. There is nothing more important that you can do to protect or expand your right to delay or decline vaccines without penalty or harassment than talking to your legislators in person and establishing a positive, respectful relationship with them. Exemption Disclosure and School ShamingThe trend to publicly disclose vaccine exemptions to shame schools with higher exemption rates has continued in 2020 where nine bills were filed in seven states. This year none of these bills passed. Promoted by those who seek to ultimately eliminate vaccine exemptions, these public disclosure bills threaten and place pressure on students with vaccine exemptions by requiring schools to publish vaccination and/or vaccine exemption rates online. These bills are promoted under the false pretense of transparency, but they are really about government-sponsored shaming of schools with students who have vaccine exemptions. The real goal of school shaming bills is to create centralized repositories of specific community level vaccine usage data that the media and public health employees use to identify and locate those who decline to receive every vaccine recommended by the CDC’s Advisory Committee on Immunization Practices. Media will use these reports in a biased manner to reflect negatively on schools with more exemptions in an attempt to solicit support for further restricting or eliminating vaccine exemptions.1 Setting up schools to be designated “winners” and “losers” in the myopic quest for a 100 percent vaccination rate with all federally recommended vaccines, these types of bills add more layers of pressure and coercion with every single dose of every single vaccine and create an environment that pits parents, children, schools and districts against each other. Arizona has had a bill filed every year since 2015 to post vaccine exemption rates. Fortunately, they have all failed to pass thanks to proactive citizen advocacy and brave legislators, who have held back these bills from moving forward. Even though these bills don’t authorize the release of individually identifiable information, the numbers of children utilizing vaccine exemptions are so small that bills like these puts the exposure of children’s identity at risk and sets them up for harassment, discrimination, and bullying. These bills need to continue to be opposed. Children Vaccinating Themselves?A very troubling area of proposed legislative changes are bills that allow minor children to be vaccinated without the knowledge or informed consent of their parents. A child is less likely than an adult parent to understand their personal and family medical history, including a history of vaccine reactions, allergies and autoimmune or neurological disorders. Minor children do not have the same kind of critical thinking skills or emotional maturity required to make a vaccine benefit-risk decision compared to an adult. In addition, if a child receives a vaccination without a parent’s knowledge or informed consent and then experiences a vaccine reaction, a parent might not recognize the potential cause of their child’s sudden decline in health. This lack of knowledge by parents could be life threatening for the child. None of the 21 bills introduced in eleven states (Colorado, Georgia, Illinois, Massachusetts, Maryland, New Hampshire, New Jersey, New York, Virginia, Vermont, Wisconsin and the District of Columbia), which attempted to grant minor children the ability to consent to vaccines on their own without parental knowledge or consent, passed. In 2019, Congress held two vaccine hearings, one on February 27th2 and another on March 5th3 and one focus of the hearing pitting children against their parents. Veteran vaccine safety and informed consent advocates with nearly four decades of experience, including time spent serving on federal advisory committees, were denied the ability to testify, but a teenager with no experience other than recently opposing his mother on social media4 for not vaccinating him was invited to testify.5 The ill-conceived concept of minor children consenting to vaccination without their parents’ consent appeared in media6 stories more frequently following the congressional hearing and used the teen’s testimony to advocate for this policy change. Medical trade groups also advanced the concept. Doctors, who are frustrated with having to spend time talking with educated parents during routine “well child” visits to answer questions and concerns about vaccines, have identified minor consent as a way to coerce children into consenting to vaccines on their own. Adolescents are vulnerable to peer and authority-figure persuasion. An opinion piece was published in The New England Journal of Medicine7 and the American Medical Association passed a resolution8 supporting state laws to allow minors to consent to vaccination. This coordinated effort resulted in 13 bills introduced in 2019 and a big jump to 21 bills introduced in 2020. Fortunately, legislators listened to parents and rejected all 34 minor consent bills filed in 2019 and 2020. Federal legislative history provides evidence that Congress never intended for a minor child to make decisions to get a vaccine without parental knowledge or consent. When the National Childhood Vaccine Injury Act9 of 1986 was passed, the Act clearly stated that before the administration of certain vaccines,10 a health care provider shall give a copy of the CDC’s vaccine information materials to either the, “the parent or legal representative of any child to whom the provider intends to administer such vaccine …” The CDC asserts the requirement that the VIS sheet is provided to the parent/legal guardian prior to vaccination of a minor child on their Q&A page on VIS sheets:11 Under the question “Is there a requirement to verify that parents/legal representatives have actually received and reviewed the VIS,” the answer is a clear and undebatable “YES.” There is no justification for the state to override a parent’s legal right to make an informed benefit and risk decision about vaccination on behalf of their minor children and hand that legal right to doctors and medical workers, who have no liability or accountability for what happens to the child after vaccination. These types of bills are a violation of parents’ constitutional right to raise their children without undue interference from the state, and each one of these bills that surfaces in state legislatures should be strongly opposed. Expanding Vaccine Exemptions and Informed ConsentHard working vaccine and health freedom advocates and open-minded legislators came together in 2020 to advocate for 78 bills in the following 25 states to expand vaccine exemptions and enhance informed consent rights:
This is a big jump from the 58 bills of this kind filed in 2019. In response to expanding vaccination schedules and overzealous forced vaccination polices implemented by day care and schools, legislators filed 20 bills in the following 12 states to expand vaccine exemptions:
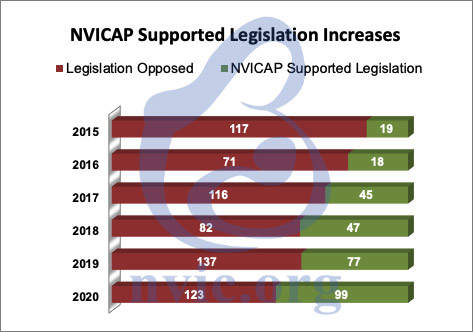
Most of the bills filed added religious or conscientious exemptions. While no bills adding vaccine exemptions for children to attend daycare and school were passed, Delaware passed a bill (HB 214) to allow veterinarians to exempt animals from rabies vaccines if the veterinarian concludes the vaccine would endanger the animal’s health. Gaps in Informed Consent on Legislators’ Radar to FixLegislators are increasingly recognizing problems created because parents are not provided enough information about potential vaccine risks and contraindications. In response, 30 bills were filed in 16 states tackling the issue of improving vaccine informed consent rights. California, Colorado, Georgia, Iowa, Illinois, Louisiana, New Jersey, New York, Ohio, Oklahoma, Pennsylvania, Tennessee, Vermont, Washington, and West Virginia all had bills filed to require additional information to be provided prior to vaccination. Nine states had legislators wanting to get better information about the increased prevalence of vaccine reactions. 11 bills were filed to require vaccine reactions to be reported to the legislature directly or through a state agency. Iowa, New Hampshire and Missouri each had a bill introduced to require death certificates to include information about vaccines administered. Also addressing gaps in informed consent, 9 bills were filed in the 7 states of Colorado, Florida, Iowa, Louisiana, Ohio, Oklahoma, and Pennsylvania that would require parents to be informed of the availability of vaccine exemptions. Often, parents do not know they have the legal right to take a vaccine exemption. Some schools don’t readily share this information and parents may be incorrectly told there is a “no shots, no school” policy that prevents unvaccinated or partially vaccinated children from enrolling in school. This can result in a child, who may be at high risk for suffering a vaccine reaction, getting vaccinated under false pressure that can lead to the child suffering a serious reaction. Other bills filed required the disclosure of certain vaccine ingredients and risks, and several bills added steps like requiring specific written permission before any vaccine could be administered. One broad groundbreaking bill in Florida entitled the “Stop Social Media Censorship Act,” would have provided civil remedies for those whose religious or political speech was censored by a social media website. While none of these bills passed, over 1,000 state legislators were educated about the failures in the informed consent process to vaccination. This education can serve as a deterrent to passing other bad bills that remove or restrict informed consent rights from being introduced in the future. Decreasing DiscriminationAn encouraging new trend is that more legislators are recognizing the significant problems caused by discrimination against those who choose to delay or decline vaccination and are willing to support legislation to stop this discrimination and bias. A total of 32 bills tackling different aspects of discrimination head on were filed. The majority of bills filed were trying to protect adult employees from any kind of penalties for refusing vaccines. This category of bills will be extremely important in 2021 as COVID-19 vaccines are rolled out and potential legislation is introduced to mandate COVID-19 vaccinations. It is critical to protect people from sanctions by employers, insurance companies, medical providers, retail establishments, and interstate travel opportunities for refusing to take a vaccine. It is not too early to talk to legislators about prefiling bills to prevent this type of discrimination ahead of the 2021 legislative session. Six bills were introduced this session to specifically prohibit insurance companies from penalizing doctors or patients when the patient did not take a recommended vaccine, while one bill in Wyoming prohibited doctors from expelling patients for vaccine refusal, and another Wyoming bill prohibited hospitals from refusing to treat individuals based solely on their vaccination status. Iowa and Michigan filed bills that would prohibit denying a foster care license based on the vaccination status of the family. Arizona, Colorado, and Oregon also tried to join the ranks of Texas with bills that prohibit either abuse claims or custody restrictions based on vaccine refusal, and Colorado’s efforts were rewarded with the passage and governor’s signature on HB 1297. This clarified that delaying or declining a vaccine by itself is not child abuse or neglect. This bill enjoyed notable bipartisan support. Colorado demonstrated that it is important not to prejudge legislators based on party affiliation for their support or opposition to a bill and it is important to sincerely educate and treat all legislators respectfully. Expanding Vaccine MandatesIn 2020, only three of the 42 bills filed to add vaccine mandates passed. Two bills were in New Jersey. Annual flu vaccines are now required for health care facility employees in New Jersey and meningococcal vaccines are now mandated for residential students at four-year colleges in New Jersey. The third and worst vaccine mandate bill to pass in 2020 was Virginia HB 1090. It gave the Governor-appointed Board of Health the authority to add federally recommended vaccines to the schedule required for school attendance (with the exception of requiring annual influenza vaccinations) without a public hearing or vote by the legislature. It also expanded the current list of required vaccines to add HPV vaccines for boys to the existing requirement for girls and added rotavirus, hepatitis A, and meningococcal conjugate vaccine requirements in conformance with recommendations of the CDC’s Advisory Committee on Immunization Practices (ACIP). This puts Virginia school children at risk of being required to receive a mandated COVID-19 vaccine once it is licensed by the FDA and recommended by ACIP for children. The Health Commissioner of Virginia has already stated that he intends to mandate12 that all Virginians get a COVID-19 vaccine when it is available. Mississippi had a failed attempt to pass a bill to mandate annual flu vaccines for school employees with no religious exemption, and New York still has two pending bills attempting to mandate flu vaccines for children in school and daycare, A2316 and S2776, that need to be watched and opposed. Five states — Illinois, Massachusetts, New Jersey, New York and Virginia — had bills filed to specifically mandate HPV vaccines for students that have not passed. New Jersey, New York, and Ohio attempted to add other adult vaccine mandates. NVIC opposes all adult mandates as a condition for employment. Vaccines are already available to those who want them. New York attempted a bill to mandate vaccines for children’s camps with no religious exemptions allowed, but it has not passed. Restricting Vaccine MandatesNVIC supported 20 bills in 13 states that would have restricted vaccine mandates. While none of these bills passed, many legislators were educated about the harm vaccine mandates can cause, and this education helped hold back the passage of dozens of bills enacting more forceful mandates. Eight bills were filed in Colorado, Idaho, Louisiana, Michigan, Minnesota and Ohio to protect employees who want to refuse vaccination requirements. These types of bills need to be filed and passed in every state. Michigan had two bills, HB 5135 and HB 5136, that would have prohibited new vaccine mandates to be issued by agency rule making. Oklahoma passed a bill in the House, but not the Senate, to require legislative approval when new vaccine mandates are added for school by the department of health. Given the threat posed by unelected and unaccountable state employees having the power to expand vaccine mandates, lawmakers in state legislatures, who have punted the responsibility of setting the vaccine schedule to health agency employees, need to take their legislative authority back so the people these mandates affect have a voice and can participate in the democratic process. Iowa and Michigan set their sights on prohibiting a requirement that foster care families vaccinate their families. While the Iowa bill died, the Michigan bill is still pending, and support could help tip this good bill over the edge to pass. Two exciting bills were introduced in Arizona (HB 2050) and South Dakota (HB 1235) to eliminate vaccine mandates, and people should consider talking to their legislators about filing this kind of bill in their own states. Brave legislators in these states recognized that vaccines are pharmaceutical products that can cause injury or death, and families should be allowed to make voluntary decisions about their use without being coerced and forced by law to vaccinate. These bills were filed as a direct result of people talking to their legislators about the harm that vaccine mandates have caused their families. Vaccine Tracking and Reporting (37 Bills)Forced inclusion, forced reporting, and opt-out electronic vaccine tracking registries and enforcement systems continue to threaten the medical privacy of citizens and their legal right to refuse federally recommended vaccines without being subjected to harassment or punishment. On the positive side, legislators are also becoming increasingly concerned about the lack of reporting and tracking of serious vaccine reactions and are trying to take steps to put this information in front of more government officials. The 2020 legislative session included 37 bills in the category of vaccine tracking and reporting that NVICAP analyzed, posted and monitored. Expanding Vaccine TrackingEighteen bills tried to expand vaccine tracking in Alabama, Arizona, Colorado, Indiana, Massachusetts, Nebraska, New Jersey, New York, and Washington. Three of these bad bills passed. This is a big improvement from 2019 where nine bills expanding vaccine tracking passed. Colorado passed SB 163 which, in addition to restricting vaccine exemptions, adds a hefty dose of increased vaccine tracking and electronic surveillance. Health care providers are required to submit all vaccines administered and also all vaccine exemption information to the state operated electronic vaccine tracking system, CIIS. Now, there is no way for public and private school students and children attending daycare to not be tracked by the health department in Colorado. Indiana passed HB 1210, which expands the current vaccine tracking system in Indiana to include additional personal health information, including newborn screening and blood lead screening. Nebraska passed LB 1183, which enacted government vaccine tracking through the Population Health Information Act. The bill was initially introduced to deal with prescription drug monitoring, but it was amended to include vaccine tracking in this new state electronic database. There is no requirement for opt-in informed consent to participate in this registry and the bill provides for any health care entity to access this information. Alabama, New Jersey and West Virginia had four additional bills that would have required vaccine providers to report to the registry, but fortunately they did not pass. All 50 states now have vaccine tracking systems13 for children and many states have expanded their systems to include adults. The Centers for Disease Control (CDC) has created a new term for vaccine tracking, surveillance, and enforcement registries so people don’t focus on and become concerned about how they are actually being used. Threats Posed by Immunization Information SystemsThe CDC now calls them Immunization Information Systems (IIS),14 which makes them seem to be more passive and less threatening. In reality, IIS represent one of the largest threats to being free to refuse any vaccination, including upcoming vaccines for COVID-19. Federal agencies are working with public health trade groups to link the registries all together15 to be able to create and access a complete personalized vaccine profile on every U.S. citizen. The Network for Public Health Law16 recently held two webinars about data sharing to support each “jurisdiction’s role in mass vaccination for COVID-19” using the Immunization (IZ) Gateway.17 The IZ Gateway is sponsored by the CDC Immunization Information Systems Support Branch and led by the U.S. Department of Health and Human Services Office of the Chief Technology Officer. Its purpose is to facilitate the sharing of everyone’s immunization status through multiple private and government entities in real time to create a virtual national immunization registry so that wherever you are, government and health care providers will know your vaccination status. This presents a huge problem for people who don’t want to have their vaccination status tracked by government or anyone else. Many states have mandatory tracking where consent is unfortunately assumed and there is no way to get out. This is sometimes initiated with the state sharing birth records to the immunization registry without a parent’s knowledge or consent for the purpose of initiating a registry file on every newborn. Some states automatically put everyone in the system but claim someone can either opt-out, or opt-out of data sharing. This is problematic for two reasons. First, because of data interoperability, every system that has access to each state registry can pull an individual’s vaccination status, store it, and release it even further before someone may have a chance to opt-out. Even if someone opts-out, the data is already out there and can’t be taken back. Second, opting-out of data sharing does nothing to protect your vaccination status from the health department who operates the registry itself. It only prevents other entities like insurance companies, health care providers or schools from accessing the information. This does little to reassure people who are concerned the information will be used to force vaccination. Many people are more concerned about what public health officials will do with this information now and in the future as the vaccine records in most IIS can never be removed. The only way to guarantee your vaccination status won’t get tracked in existing vaccine tracking registries by your state and used to penalize you or enforce vaccination is for your state to legislate explicit opt-in consent for inclusion into the registry and for the release of data out of the registry. Also, the option for complete personal vaccine data purging from the registry and all other health department files should be enacted for those who want their personal information removed from the registry after it has been included. Texas and Montana are the only states that require opt-in informed consent.18 If you do not live in either of these states, laws need to be changed to prohibit any collection or sharing of your medical/vaccine records without your expressed written informed consent. With impending controversial COVID-19 mass vaccination programs, limiting personal health information that is collected and shared with IIS is critical. Strong opposition to mandatory inclusion, assumed consent, and opt-out vaccine tracking systems is needed. Reaching a 100% vaccine compliance rate by all children and adults is the goal of these electronic vaccine tracking systems. Expanding Vaccine Reaction Reporting and TrackingOn the other side in a positive new trend, there were 14 bills requiring the reporting or recording of vaccine reactions. California, Iowa, Louisiana, New Hampshire, New Jersey, Rhode Island, Vermont and Washington had 11 bills requiring that reports of vaccine reactions be sent to the legislature or the state. Iowa, New Hampshire and Missouri took on the heart wrenching topic of infant deaths following vaccination and had three bills requiring vaccine information to be recorded on death certificates or to be reported to the Vaccine Adverse Event Reporting System (VAERS). While none of these bills passed, legislators were educated about the lack of public transparency about real vaccine reactions and deaths and these bills were a great first step at trying to change that. Emergency PowersArizona and Pennsylvania had two bills that attempted to expand emergency powers by the state but they did not pass. In 2021, we can expect many more bills trying to expand emergency powers, as well as curtail abuses of emergency powers, in direct response to the COVID-19 pandemic of 2020. These bills will need to be watched carefully. Most states lack sufficient vaccine exemptions to protect citizens from forced vaccination in times of declared public health emergencies. Now would be a good time for people to review their state emergency powers laws to look for problems and talk to their legislators about filing bills before the 2021 legislative sessions to expand vaccine exemptions for all state residents during a declared public health emergency. This is especially important for those who have concerns about potential mandates for COVID-19 or influenza vaccines. Authorizing More Professions to Administer More VaccinesOne of the most successful areas where we worked with families in the states was in the area of bills that proposed to expand the authority to pharmacists and others to administer vaccines to children. There were 22 bills filed in 14 states (Arizona, California, Florida, Iowa, Louisiana, Maryland, New Hampshire, New York, Ohio, Oklahoma, Pennsylvania, South Carolina, Virginia and Wisconsin) to allow pharmacists and other types of medical professions to administer vaccines to young children. Four of the 22 bills attempted to expand vaccine administrators to other professions outside of pharmacists. Ohio had a bill trying to allow podiatrists to give flu vaccines to anyone 7 years old and up, Oklahoma tried to get paramedics to give vaccines, and Wisconsin tried to give authority to dentists to administer vaccines. Fortunately, none of these bills passed but it is easy to see how other professions want a piece of the almost $18 billion U.S. vaccine market in 2020,19 and how that could lead to more “gatekeepers” instituting policies that refuse services to the unvaccinated. In terms of expanding a pharmacist’s ability to give vaccines, both New Hampshire and New York passed controversial futuristic bills allowing pharmacists to vaccinate for COVID-19 once a vaccine becomes available. Other than the two COVID-19 expansions bills, the only other bill of this type that passed was in Florida, but the offending language allowing pharmacists to vaccinate children was completely removed from the bill thanks to strong opposition. Unfortunately, the federal government stepped in and overrode the states on the issue of pharmacists being given the authority to vaccinate young children. State legislatures were completely circumvented by an action taken by the Secretary of Health and Human Services, Alex Azar.20 On August 24, 2020, the Federal Register published Mr. Azar’s amendments21 to the declared emergency for COVID-19 issued under the Public Readiness and Emergency Preparedness (PREP) Act for Medical Countermeasures Against COVID-19. Countermeasures include vaccines for ACIP-recommended vaccines and this amendment now allows pharmacists to administer every ACIP-recommended vaccine to all children 3 years old or older, regardless of what each state law limits. This is a significant abuse of federal power. Pharmacists Are Not DoctorsStates have been deliberately cautious about limiting the types of vaccines and ages of children which pharmacists are allowed to vaccinate. The actions of Mr. Azar, who is a former CEO of the U.S. pharmaceutical company Eli Lilly, and a former pharmaceutical lobbyist,22 illustrate the problems created by the revolving door between the pharmaceutical industry and government agencies. Pharmacists administering vaccines in the corner drug store or grocery store pharmacy to minor children and toddlers trivializes very real vaccine risks and the potential for serious reactions. Pharmacists are not doctors and 20 hours of required training23 for pharmacists to be able to administer all childhood vaccines cannot substitute for the knowledge and practical experience that doctors and nurses have administering vaccines. Pharmacists are not as knowledgeable about diagnosing the difference between cardiac arrest, anaphylaxis and fainting and most pharmacies don’t have lifesaving defibrillators. The limited training pharmacists get in vaccines will not be able to cover all the contraindications for the 57 different unique vaccines available24 now in the U.S. or the nearly 260 vaccines in development.25 Ensuring informed consent and accurate screening to consider family and individual medical histories will be challenging in the back of a pharmacy or a grocery store. Certain allergies, fevers, weakened immune systems, seizures, pregnancy, Guillan-Barre Syndrome and other reactions post vaccination are all reasons listed on the CDC’s Vaccine Information Statements indicating a possible reason to not vaccinate. It is also a stretch to think pharmacists are going to report reactions to the Vaccine Adverse Events Reporting System (VAERS)26 or warn parents about the statute of limitations and instructions for filing a claim with the National Vaccine Injury Compensation Program,27 which has paid out over $4.4 billion28 to vaccine victims. Rules Carry the Same Effect as LawAdministrative rules, while not law, carry the same effect as law. State legislatures delegate rule-making authority to the state agencies, boards of health, or health commissioners tasked with implementing state law, however, they are not supposed to change or add to what is in statute. As more concerned citizens have made significant impact in stopping bad vaccine bills, some state health departments have turned to the rule process to add more mandates or restrict vaccine exemptions. Additionally, there has been a trend in recent years for some state legislators who are influenced by the medical trade lobby to move the task of setting vaccine mandates or setting the criteria for vaccine exemptions completely out of the legislature and into the hands of state employees. It is a widespread problem that many state agencies abuse their power and write rules that go beyond the scope of the state statute they are implementing. Many state’s administrative procedures acts do not give the average citizen sufficient opportunities to give feedback that will be sincerely considered. Because state employees are not elected, state residents don’t have any recourse to remove them from their jobs as they are able to do with elected legislators who restrict or eliminate rights. In the 2020 legislative session, NVIC Advocacy tracked and issued action alerts on proposed administrative rule changes in four states, Oklahoma, Washington, Wisconsin, and Wyoming. NVIC Advocacy team members and like-minded groups worked together in these states to stop these four rule changes. The Oklahoma rule change would have restricted vaccine exemptions by requiring the completion of a mandatory health department educational presentation in order to obtain a religious or personal belief exemption. Strong opposition to this attempted restriction to exemptions helped ensure that the rule was amended to remove this burden on exemptions in Oklahoma. Washington, Wisconsin and Wyoming proposed new vaccine mandates through rule. Local vaccine informed consent and health freedom groups came through in large numbers attending public comment sessions and submitting comments, engaging more families concerned about expanding vaccine schedules and communicating with legislators to ask them to oppose the rule changes as well. This resulted in all of these proposed rule changes for new vaccine mandates being withdrawn. Proposed rule changes are typically published in state registers. It is important to watch the state health and education agency registers for proposed rules regarding vaccine requirements and exemptions. Links to these state registers are available on the NVIC law pages. Sometimes contacting your legislators about proposed rules that force more vaccines or restrict vaccine exemptions can be helpful if the legislator contacts the agency and ask them to back off. Legislators, especially those who sit on powerful appropriation committees setting state budgets, can have more of an influence than the average citizen. NVIC is opposed to unelected unaccountable state employees setting required vaccine schedules. A good bill to file in states where the legislature has abdicated its power to control what vaccines are mandated on its citizens would be to repeal these laws and return control back to legislators who must face voters at the ballot box. Comparing Recent Sessions to 2020232 bills represent the most proposed vaccine-related bills NVIC has recorded in the history of the NVIC Advocacy Portal, surpassing the previous all-time high of 221 bills introduced in 2019. It is important to note that four states (Montana, Nevada, North Dakota and Texas) meet biennially to consider new bills and do not hold a legislative session in even years. It is remarkable that this record number of vaccine-related bills were proposed with these four states not participating in the 2020 legislative session. The number of states proposing bills in 2020 that affected NVIC’s mission remained similar to last year: 39 and the District of Columbia compared to 40 and the District of Columbia in 2019. There were fewer bills that NVIC opposed in 2020 compared to last year (123 versus 137). There were more bills filed that NVIC supported in 2020 than in any other session. NVIC supported 99 bills this session, which is 22 more positive bills than the previous record-breaking number of 77 bills NVIC supported in 2019. Enlightened legislators are not only listening to concerned constituents in greater numbers, many more are continuing or beginning to resist aggressive lobbying efforts by the vaccine industry, medical trade and other groups, whose positions and profits benefit from laws that force children and adults to use every vaccine sold by pharmaceutical companies and recommended by public health officials. Only eight bad vaccine bills passed out of the 123 that NVIC opposed in the 2020 legislative session, which was 10 less than the 18 bad vaccine bills that passed last year. Individual citizen involvement in the legislative process, through personal communications and education of legislators, continues to make a significant impact year after year on the outcomes of vaccine related bills in state legislatures. NVIC predicts that the continued attack on vaccine exemptions and bills to expand emergency powers and mandate fast tracked COVID-19 vaccines after they are licensed and recommended by the federal government will drive even more Americans in every state to get more involved in the legislative process at every level in the years to come. 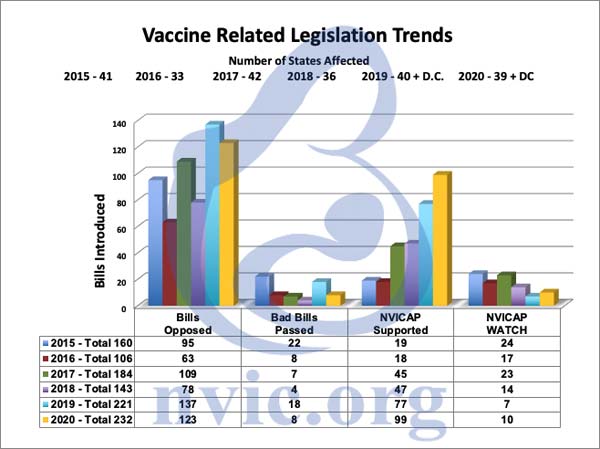
What Can You Do?NVIC expects that the vaccine industry and their medical trade association partners will step up lobbying efforts to restrict or remove vaccine exemptions in 2021 since so many of their bills failed in 2020. Please become a registered user of the free online NVIC Advocacy Portal and check in often to learn about ways to personally educate your legislators when vaccine bills that affect your rights are moving in your state. Please encourage your family and all of your friends to do the same. Clearly your efforts are making a much more significant difference than the mainstream media and those pushing “no exceptions” forced vaccination policies and laws are willing to admit, and your active participation is vital to protecting informed consent rights and vaccine choices in America. If you see inaccurate information in the media, please take the time to respond by making a constructive comment online. You can also email the journalist or call the media outlet and provide accurate, well referenced Diseases and Vaccines information and accurate state vaccine law information, which you can find on our website NVIC.org. NVIC’s illustrated and fully referenced Guide to Reforming Vaccine Policy and Law is another good vaccine education tool for legislators and friends and family, too. The same holds true if you are censored online for providing accurate information about vaccination, infectious diseases and health. Contest it and educate those doing the censoring. The information seeds you plant today can make a difference tomorrow and into the future. Yes, the challenges are great but so are the opportunities to educate and empower legislators and residents of every state to defend vaccine freedom of choice. NVIC is committed to continuing to make that happen and we look forward to working with you through the NVIC Advocacy Portal to help you protect vaccine informed consent rights in your state in 2021 and beyond. from http://articles.mercola.com/sites/articles/archive/2020/09/24/nvic-2020-annual-report-vaccine-legislation.aspx While most mainstream media pundits and American health authorities remain mum about the influence of nutrition and lifestyle on the risks of COVID-19 and its prognosis, more than a dozen states in Mexico have decided to combat the pandemic by banning the sale of junk food to minors. Mexico Bans Junk Food to Curtail COVID-19 Death TollAs reported by NPR, September 14, 2020:1
Adults are also urged to cut back their consumption of junk food to curtail their risk of COVID-19 and other health issues. This includes the consumption of soda, which assistant health secretary Hugo López-Gatell has referred to as "bottled poison."2,3 Legislators are still pondering how to enforce the ban, but according to NPR, punishment for sale of junk food to minors could potentially include fines or even jail time. López-Gatell is reportedly considering making the ban a permanent law in order to protect the health and well-being of Mexican youth moving forward. This would be no easy task, he admits, considering the powerful commercial interests at play. Critics also point out that, in all likelihood, the ban will simply shift business from grocery stores to unregulated street vendors. Interestingly, when NPR interviewed teenagers around Mexico City and Oaxaca state, they found most “knew about health problems related to junk food” and seemed receptive to the ban. One 16-year-old girl said, “I'd be frustrated at first if I couldn't buy a Coke, but I'd adapt. And maybe I'd think twice and buy fruit or something healthy instead." Nutrition Plays an Important Role in COVID-19 SusceptibilityAs reported in “Junk Food Companies Responsible for COVID-19 Susceptibility,” underlying health conditions such as obesity, heart disease and diabetes have emerged as key factors in COVID-19 fatalities. In one study,4,5 more than 99% of people who died from COVID-19-related complications had underlying medical conditions. Among those fatalities, 76.1% had high blood pressure, 35.5% had diabetes and 33% had heart disease. Another study6 revealed that among 18- to 49-year-olds hospitalized due to COVID-19, obesity was the most prevalent underlying condition, just ahead of hypertension. Processed foods, junk foods and soft drinks are key culprits in the development of these chronic diseases, and therefore have a key role to play in COVID-19 hospitalizations and deaths. London-based cardiologist Dr. Aseem Malhotra has been among those warning that poor diet can increase your risk of dying from COVID-19. He told BBC that ultraprocessed foods make up more than half the calories consumed by the British, and if you suffer from obesity, Type 2 diabetes and high blood pressure — all of which are linked to poor diet — your risk of mortality from COVID-19 increases tenfold.7 Malhotra also noted8 that eating nutritious foods for even one month could help you lose weight, put Type 2 diabetes into remission and improve your health considerably, thereby improving your chance of survival should you contract COVID-19. Dr. Robert Lustig, Emeritus Professor of pediatrics in the division of endocrinology at the University of California, San Francisco, has also been outspoken about the connection between diet and COVID-19 risks, stating:9
Even Mild Obesity Increases Risk for COVID-19 ComplicationsImportantly, even mild obesity can have significant implications for COVID-19. According to Italian researchers who analyzed10 data from 482 COVID-19 patients, “Obesity is a strong, independent risk factor for respiratory failure, admission to the ICU and death among COVID-19 patients,” and the extent of risk is dependent on your level of obesity. In a press release, lead author Dr. Matteo Rottoli stated:11
Specifically, patients with mild obesity had a 2.5 times greater risk of respiratory failure and a five times greater risk of being admitted to an ICU compared to nonobese patients. Those with a BMI of 35 and over were also 12 times more likely to die from COVID-19.12 British Report Links Obesity to COVID-19 Severity and DeathSimilarly, a July 2020 report13 by Public Health England described the results of two systematic reviews,14 one of which showed that excess weight worsened COVID-19 severity, and the other that obese patients were more likely to die from the disease compared to nonobese patients. Here too, the risk of hospitalization, intensive care treatment and death all progressively increased along with BMI. Compared to healthy weight patients, patients with a BMI above 25 kg/m2 were:
Yet another study15,16 published May 2, 2020, on the preprint server medRxiv found obesity doubles your risk of being hospitalized for COVID-19. According to the authors:17
Pandemic Has Highlighted Role of Junk Food in HealthIn an editorial18 published in the BMJ, three researchers cited the role of the food industry in driving up rates of obesity and ultimately causing more COVID-19 deaths. According to the authors, “It is now clear that the food industry shares the blame not only for the obesity pandemic but also for the severity of COVID-19 disease and its devastating consequences.” They not only called on the food industry to stop promoting unhealthy food and drinks immediately, but also called on governments to force reformulation of junk foods to better support health. As noted by Bill Maher in the video above, obesity has always killed us, albeit slowly. “Mixed with COVID, it kills you fast,” he says. So far, Mexico appears to be the only nation that has taken the matter seriously enough to actually implement an all-out ban on junk food for children and teens. Other noteworthy exceptions include the town of Huntington, New York, where town officials have urged residents to “go on a diet because [with] COVID-19, you’re twice as likely to have a poor outcome if you’re obese.” The U.K. is also targeting obesity as part of the country’s coronavirus prevention strategy by restricting junk food ads.19 July 23, 2020, Prime Minister Boris Johnson announced he intends to ban TV junk food advertising before 9 p.m. and limit in-store promotions. Online ads for unhealthy foods may also be banned.20 Studies Stress Nutrition in Fight Against COVID-19Two additional studies are worthy of note. The first, published in the May 2020 issue of Pakistan Journal of Medical Sciences,21 points out that “Optimal nutrition and dietary nutrient intake impact the immune system, therefore the only sustainable way to survive in current context is to strengthen the immune system,” and that “A proper diet can ensure that the body is in proper state to defeat the virus.” To optimize your chances of surviving COVID-19 and minimizing its symptoms, the authors provide both dietary guidelines and good food practices to minimize the risk of food contaminants. Included in the dietary guidelines are recommendations to:
Unfortunately, the guidelines include the recommendation to avoid healthy saturated fats such as butter, coconut oil, cheese, ghee and cream, and to use unsaturated fats only. While some unsaturated fat sources are perfectly healthy, such as avocados, fish and nuts, others really should be avoided. Industrially processed seed oils are fats to be diligently avoided and this includes oils like soybean oil, canola oil and corn oil. The second study, published in the July 2020 issue of Brain, Behavior and Immunity, notes that:22
My Dietary RecommendationsIt really did not take long before it became apparent that the COVID-19 pandemic was illustrative of a far more widespread pandemic, namely that of insulin resistance. All of the comorbidities that dramatically increase your COVID-19 risks (including your risk of symptomatic COVID-19 illness, hospitalization and complications resulting in death) are rooted in insulin resistance. Remove the insulin resistance, along with vitamin D deficiency, and very few people — except for very old and frail individuals — would be at significant risk from SARS-CoV-2 infection. So, it really is high time to start looking at how we can improve our health in general, and avoid insulin resistance in particular. A healthy population simply isn’t going to be as vulnerable to infectious diseases like COVID-19. Aside from the general dietary recommendations listed above (with the exception of the recommendation to replace saturated fats with soy, canola and corn oils), I recommend: • Adopting a cyclical ketogenic diet, which involves radically limiting carbs (replacing them with healthy fats and moderate amounts of protein) until you're close to or at your ideal weight. This includes avoiding all ultraprocessed foods and also limiting added sugars to a maximum of 25 grams per day (15 grams a day if you're insulin resistant or diabetic). This will allow your body to start burning fat rather than carbohydrates as its primary fuel and increase the sensitivity of your insulin receptors. Once you have regained your ideal body weight, then you can cycle carbs back in a few times a week. One of the best books written on this subject is my classic “Fat for Fuel.” • Restricting your eating window to six to eight hours each day, making sure to eat your last meal at least three hours before bedtime. This is known as time-restricted eating or intermittent fasting, and is a powerful intervention to reduce insulin resistance and restore metabolic flexibility. Additionally, get regular exercise each week and increase physical movement throughout your waking hours, with the goal of sitting less than three hours a day. Making sure you’re getting sufficient sleep (typically eight hours for most adults) and tending to your emotional health are also important factors that can influence your weight, general health and immune function. from http://articles.mercola.com/sites/articles/archive/2020/09/24/mexican-junk-food-ban.aspx From the beginning, researchers and scientists have been scrambling to find answers to a multitude of questions that affect patients with SARS-CoV-2. Scientists want to know how the virus infects human cells, how it is spread and what might be done to effectively treat a population that does not respond consistently. In other words, there are some people who are either asymptomatic or have a mild illness and others who develop significant disease and die from the virus. Experts are asking what causes one person’s immune system to go out of control and not others’? Interferon Plays a Critical Role Controlling CytokinesThe body uses type 1 interferon in response to many viral infections.1 As scientists have gotten a clearer understanding of how the virus affects the human immune system early in the disease, they have begun to theorize that interferons may be able to counter the process and prevent the development of severe illness.2 Interferons are a family of proteins produced by the immune system. Human-type interferons have also been commercially produced using recombinant DNA for treatment against viral infections, some cancers and multiple sclerosis.3 The objective is to change the immune system’s response to bacteria, cancer and viruses. Natural interferon regulates the action of genetic material that secretes cellular proteins affecting growth.4,5 The theory is that building a stronger immune system will result in directing a strong defense against the virus and alleviating the cytokine storm. In the 1990s interferon was used to treat hepatitis C. However, the cure rate was 30% or less and the side effects were significant, including psychiatric issues, liver problems and depression that sometimes led to suicide.6 Other side effects included fever, muscle aches, headaches and other flu-like symptoms.7 Dr. Anthony Fauci, director of NIH’s National Institute of Allergy and Infectious Diseases (NIAID), calls interferon “the best soldiers, as it were, of the innate immune system."8 Several trials are currently underway to evaluate the effectiveness of interferon in patients with COVID-19. These trials are the result of studies demonstrating that individuals with the worst cases of coronavirus have the weakest interferon response. People With Severe Disease Have Impaired Interferon ResponseOne team conducted an immune analysis on 50 patients who presented in various stages of the disease. They found that those with severe and critical illness had an impaired interferon type 1 response.9 Another group from New York's Mount Sinai Hospital reported similar results in the journal Cell after studying the virus in infected cells in the lab, humans and ferrets.10 Their data showed low levels of interferon types 1 and 3 were associated with higher levels of chemokines. One team used immune cells from the blood of individuals who had severe disease. Using mass cytometry, they assessed the immune response in patients with confirmed disease.11 As reported in the Washington Post, when the immune cells were challenged with bacteria and viruses the normal reaction of producing defense of molecules, including interferons, did not occur.12 British company Synairgen published In a July 2020 press release, British company Synairgen suggested results from a randomized clinical trial using inhaled interferons could be used to reduce the potential risk of developing severe disease.13 While these results are promising, it's important to note that the trial was limited and the results have not yet been peer-reviewed or published. One month later, the NIAID announced they were sponsoring a clinical trial to test interferon in hospitalized patients.14 Scientists are currently recruiting for the trial and hope to evaluate data from 1,000 patients across 100 hospitals worldwide. The patients in the study will be getting remdesivir, the antiviral approved by the FDA in spring 2020. Fauci commented on the combination:
New Trial Couples Interferon With RemdesivirResearchers are seeking answers as to whether interferon will give added value to the antiviral agent remdesivir. However, not all scientists think there may be positive results. Marta Gaglia is a microbiologist at Tufts University. She spoke with a reporter from The Washington Post, saying, “In principle, you could think, why don’t we just give it to everybody who has a viral infection ever. But in reality, it has proven less effective than we would like.”15 The results from remdesivir studies have not been positive, either. For instance, in one study published in the New England Journal of Medicine, the endpoint measurements were changed throughout the study.16 At the conclusion the single primary outcome measure was the number of days to recovery.17 All other criteria were moved to secondary outcome measurements. This trial was also funded by the NIAID, which Fauci directs. Although the release generated enthusiasm, there were significant issues with the design and consequently the data, which I discussed in “The New COVID-19 Medication Isn't Backed by Results.” A second study published in The Lancet concluded the drug was “not associated with statistically significant clinical benefits.”18 As the head of NIAID, Fauci has a vested interest in the development of the antiviral drug remdesivir. As it was, when he declared the results of the NEJM study to be “highly significant,”19 it suggests he should have also declared a conflict of interest in the use of the drug in the U.S. When he was asked about the results of the study, which was stopped because of serious adverse events related to the drug, Fauci disregarded the evidence as “not adequate.”20 Despite scientists' concerns over the veracity of the studies, the U.S. FDA issued an emergency use authorization for it May 1, 2020, which opened the door for compassionate use of the questionable drug.21 Retroviruses May Play a Role in COVID-19 IllnessOne reason interferon may have a more positive result in the treatment of COVID-19 than they had with SARS or MERS is the potential that the SARS-CoV-2 virus is not completely responsible for the severe disease that affects a small percentage of the population. In my interview with cellular and molecular biologist Judy Mikovits, Ph.D., she discusses the potential that the SARS-CoV-2 virus activates a retrovirus in the body. You can see the interview in my article, “Judy Mikovits Suggests Retroviruses Play a Role in COVID-19.” The genetic code for a retrovirus is in ribonucleic acid (RNA), rather than in deoxyribonucleic acid (DNA). The virus uses an enzyme, reverse transcriptase, to transform the single strand of RNA into a double strand of DNA.22 The enzyme is in the host cell where the virus replicates and then spreads throughout the body. As Mikovits describes, the key to health is to keep these viruses silent.23 She believes her data show that the SARS-CoV-2 virus is not the cause of COVID-19 but rather the catalyst to its expression, as it activates a dormant XMRV retrovirus found in some people. XMRV stands for “xenotropic murine leukemia virus-related virus.” Xenotrophic refers to viruses that only replicate in cells other than those of the host species. So, XMRVs are viruses that infect human cells yet are not human viruses.24 In my interview with her, Mikovits describes how many of the current vaccines may be contaminated with this retrovirus. As some vaccine viruses are grown in contaminated animal cell cultures, the retroviruses are then transferred to the genetic material of the vaccine virus. This may well explain the varying effect the virus has, creating severe disease in some and asymptomatic or mild illness in others. Consider These Options to Reduce the Severity of DiseaseIn addition to hand-washing and maintaining overall health, there are further strategies to consider. These are approaches you can use to help reduce the risk you'll get sick or reduce the severity of the illness if you do get sick, without depending on prescribed medications. As I've written before, optimizing your vitamin D level is probably the easiest, least expensive and most beneficial strategy you can use to minimize your risk of COVID-19 and other infections. Unfortunately, there's a pandemic of vitamin D deficiency across all age groups.25,26,27 The report I wrote on vitamin D and the prevention of COVID-19 is a resource to help you understand the importance of optimizing it for healthy immune function. Evidence continues to be published demonstrating that vitamin D levels are an independent indicator of the risk for infection and hospitalization.28 There are many health experts who are getting significantly positive results using hydroxychloroquine in combination with zinc and azithromycin.29 However, you have access to a similar combination at home using quercetin and zinc. Quercetin is a natural antihistamine and anti-inflammatory30 that also functions as a zinc ionophore.31 In other words, it helps zinc to enter the cells and stem the tide of viral replication. This works not only in lung tissue but also in endothelial cells, which affect symptoms outside the pulmonary system.32 Zinc deficiencies are commonly found in older adults and in those who are obese, have diabetes or atherosclerosis.33 Likely not by coincidence, these are some of the same populations who have a higher risk of severe disease.34 I recently interviewed Dr. David Brownstein, who has a clinic outside of Detroit. He has successfully treated more than 100 patients with COVID-19 using nebulized hydrogen peroxide. You can see the interview in “How Nebulized Peroxide Helps Against Respiratory Infections.” I first wrote about using nebulized hydrogen peroxide in April 2020 and since then have received some impressive testimonials of its effectiveness from friends and acquaintances who got severely ill and used it. Brownstein was an early adopter of both vitamin D optimization and nebulized peroxide. He's been using nebulized peroxide in the clinical setting for 25 years and with each revision of his protocol, his patients have appeared to fare better than those before them. For a couple of months, Brownstein posted some video interviews with his patients in which they told their story. However, he removed them after receiving a warning letter from the Federal Trade Commission in which they stated that since there was no established prevention, treatment or cure for COVID-19, any mention thereof is in violation of FTC law. from http://articles.mercola.com/sites/articles/archive/2020/09/23/interferon-investigated-for-covid-treatment.aspx Over the past few months, several investigations have highlighted the apparent influence of vitamin D in COVID-19 incidence, severity and mortality. Interestingly, recent genetic analysis has produced a novel hypothesis1 that helps explain the unusual disease progression of COVID-19. The hypothesis,2 published in the journal eLife in July 2020, specifically identifies bradykinin, a blood pressure regulating chemical controlled by your renin-angiotensin system (RAS), as a primary culprit. As reviewed in greater depth in "Bradykinin Hypothesis Explains COVID-19 Complexities," the lethality of COVID-19 may be due to the virus' ability to induce a bradykinin storm. The effects of the virus on your RAS also adds further support to the recommendation to optimize your vitamin D. In fact, the researchers who came up with the novel bradykinin hypothesis stress the usefulness of vitamin D, as it plays an important role in the RAS system3,4,5,6 and suppresses the biosynthesis of a compound called renin (REN), thereby preventing a deadly bradykinin storm. Conversely, if you are vitamin D deficient, your renin expression is stimulated, and based on the latest data, that may render you more prone to bradykinin storm. Other studies have also emerged in recent weeks, showing that raising patients' vitamin D levels has a dramatic and beneficial effect on COVID-19 outcomes. Vitamin D Massively Reduces ICU AdmissionsAmong them is a pilot randomized clinical study7,8,9 published online August 29, 2020, which found hospitalized COVID-19 patients in Spain who were given supplemental calcifediol (a vitamin D3 analog also known as 25-hydroxycholecalciferol or 25-hydroxyvitamin D) in addition to standard of care — which included the use of hydroxychloroquine and azithromycin — had significantly lower intensive care unit admissions. Patients in the vitamin D arm received 532 micrograms of calcifediol on the day of admission (equivalent to 106,400 IUs of vitamin D10) followed by 266 mcg on Days 3 and 7 (equivalent to 53,200 IUs11). After that, they received 266 mcg once a week until discharge, ICU admission or death. Of those receiving calcifediol, only 2% required ICU admission, compared to 50% of those who did not get calcifediol. None of those given vitamin D supplementation died, and all were discharged without complications. CDC Warns of Second Wave of COVID-19In the video above, NBC News interviews Michael Osterholm, virologist and director of the Center for Infectious Disease Research and Policy at the University of Minnesota in Minneapolis, about the prospect of a second wave of COVID-19. According to Osterholm, we likely have another 12 to 14 months of "a really hard road ahead of us." While Swedish statistics suggest the virus can and is dying off naturally, Osterholm believes cases will again rise as we move into fall and winter. Even if a vaccine does become available, it will take months to vaccinate the population, he notes. Chief epidemiologist in charge of Sweden's coronavirus response, Anders Tegnell, has stated12 he does not believe Sweden will see a second wave with widespread contagion as the country is seeing a rapid decline in positive tests, indicating herd immunity is being achieved.13 That said, there are still open questions as to how long natural immunity might last.14 Some evidence points to months,15 while other data point to several years.16 Then there are the data suggesting herd immunity for COVID-19 occurs at much lower rates than normal. As reported17 by Dr. James Hamblin in The Atlantic, infectious disease modeling by Gabriela Gomes, who specializes in nonlinear chaos dynamics, "selective depletion" of individuals susceptible to infection can rapidly reduce viral spread, and in the case of SARS-CoV-2, models suggest the threshold for herd immunity may occur below 20% of the population. Yet other data18,19,20,21 suggest certain antibodies against other coronaviruses, such as the common cold, appear to provide some protection against SARS-CoV-2 as well, such that a majority of people may already have some level of immunity. So, there's a variety of "moving parts" that still need to be nailed down before we can come to any firm conclusions about future risks. Vitamin D Versus VaccineWhile Osterholm22 and other health officials are still focused on getting people onboard with vaccination, both against influenza and COVID-19, no one at the federal level has as of yet addressed the elephant in the room, which is vitamin D deficiency and its impact on these infections. Importantly, influenza vaccination has been shown23,24 — by the Department of Defense, no less — to increase the risk of subsequent coronavirus infections by 36%. If we are to follow the science, as Osterholm says, then we should not be so quick to overlook such findings. Then, of course, there's the issue of whether a safe and effective COVID-19 vaccine is achievable. I've discussed the reasons for why I believe COVID-19 vaccines will fail in several previous articles. Vitamin D optimization, in contrast, is already known to be both safe and effective against not only influenza but also COVID-1925,26,27 and other respiratory infections.28 According to a 2017 systematic review29,30,31 published in The BMJ, vitamin D supplementation protected against acute respiratory tract infection. The number needed to treat (NNT) was 33, meaning 33 people had to take the supplement in order to prevent a single case of infection. Among those with severe vitamin D deficiency at baseline, the NNT was 4. Meanwhile, a systematic review32 by the Cochrane Database of Systematic Reviews found that to prevent one case of influenza-like illness (defined33 by the World Health Organization as an acute respiratory infection), the NNT for inactivated vaccines was 40. To prevent a single case of confirmed influenza, the number needed to vaccinate (NNV) was 71. Vitamin D Is an Important Modifier of COVID-19 RiskIn a November 1, 2020, commentary34 in the journal Metabolism Clinical and Experimental, JoAnn Manson and Shari Bassuk call for the elimination of vitamin D deficiency to effectively squelch the COVID-19 pandemic, noting that 23.3% of the total U.S. population have insufficient or deficient vitamin D levels, with people of color having disproportionately lower levels than non-Hispanic whites. They list several types of studies showing vitamin D deficiency is "an important modifiable risk factor for COVID-19," including:35 • Laboratory studies that demonstrate how vitamin D helps regulate immune function and the RAS, and modulate inflammatory responses to infection. • Ecologic studies showing populations with lower vitamin D levels or lower UVB radiation exposure have higher COVID-19 mortality,36,37,38 and the fact that people identified as being at greatest risk for COVID-19 hospitalization and death (people of color, the elderly, nursing home residents and those with comorbidities such as obesity, vascular conditions and chronic kidney disease) also have a higher risk of vitamin D deficiency. • Observational studies showing low vitamin D levels are associated with a greater risk of testing positive for SARS-CoV-2 and contracting acute respiratory infections. According to a September 3, 2020, JAMA study,39,40 people who tested positive for SARS-CoV-2 were 1.77 times more likely to be deficient in vitamin D than those who tested negative for the virus — a statistically significant difference. CTV News, which reported the JAMA results, also pointed out that:41 "The connection between vitamin D and other respiratory illnesses is well known. According to the World Health Organization,42 vitamin D deficiency has been linked to pneumonia, tuberculosis and bronchiolitis," and that "research43 out of New Orleans found 100% of its sickest COVID-19 patients were deficient in vitamin D." • Randomized clinical trials showing vitamin D inhibits respiratory tract infections, especially in those with lower vitamin D levels at baseline. Vitamin D Protects Your LungsA 2020 GrassrootsHealth study published in the journal Nutrients44 describes how vitamin D can reduce the risk of both influenza and SARS-CoV-2 infection by lowering the viral replication rate and reducing the pro-inflammatory cytokines that damage the lungs, leading to pneumonia. Vitamin D also helps increase concentrations of anti-inflammatory cytokines that may help protect your lungs. The researchers recommended those at risk for COVID-19 take:
Vitamin D and COVID-19 ComorbiditiesVitamin D may also help protect against COVID-19 by beneficially impacting many of the comorbidities associated with poor COVID-19 prognosis. In an August 2020 paper45 published in the NSF Journal, the authors review the "fatal relationship" between vitamin D deficiency in combination with comorbidities in COVID-19 patients, noting that:
How Vitamin D Helps Modulate SARS-CoV-2 InfectionThis brings us back to where I started. While this NSF Journal study does not make reference to bradykinin storm being part of the disease progression and lethality of COVID-19, it does review how vitamin D impacts your RAS (which regulates bradykinin), and how your RAS in turn plays a role in the progression of SARS-CoV-2 infection:46
The NSF Journal paper goes on to review the connections found between the RAS, vitamin D levels and a list of comorbidities shown to worsen COVID-19 outcomes, including high blood pressure, cardiovascular diseases, obesity, Type 2 diabetes and ARDS. It also reviews how vitamin D levels, RAS function and cytokine storms are interconnected. The authors state, in conclusion:47
SummaryTo summarize what the NSF and eLife journals tell us, when your vitamin D is low, your risk of COVID-19 complications and death increases because your renin expression is stimulated. High renin increases both cytokines and bradykinin, placing you at risk for increased inflammation and oxidative stress resulting in both cytokine storm (as discussed in the NSF paper48) and bradykinin storm (as discussed in the eLife paper49). Considering cytokine and/or bradykinin storms are key factors in COVID-19 mortality, it seems reasonable to conclude that anything that can help modulate and prevent these devastating storms would be of significant value. As of right now, the one thing we know can do that is vitamin D. In addition to that, vitamin D lowers viral replication,50 boosts your overall immune function by modulating both innate and adaptive immune responses, reduces respiratory distress,51 improves overall lung function and helps produce surfactants in your lungs that aid in fluid clearance.52 Vitamin D also lowers your risk of comorbidities associated with poor COVID-19 prognosis, including obesity,53 Type 2 diabetes,54 high blood pressure55 and heart disease.56 In my view, there's every reason to believe vitamin D optimization will help lower your risk of COVID-19 complications and death, and no reason to dismiss this strategy. Optimize Your Vitamin D Level NowMy #StopCOVIDCold campaign seeks to raise awareness about the importance of vitamin D optimization to prevent a resurgence of COVID-19 hospitalizations and deaths. As temperatures and humidity levels drop — two factors that influence the viability of the virus in air and on surfaces — it's quite likely we'll see a reemergence. But a surge in positive tests, by itself, should not be cause for panic. Remember, a vast majority of so-called "cases," meaning positive tests, remain asymptomatic. I believe raising vitamin D levels among the general public can go a long way toward increasing the number of people who have no symptoms or only mild illness. Now is the time to check your vitamin D level and start taking action to raise it if you're below 40 ng/mL. An easy and cost-effective way of measuring your vitamin D level is to order GrassrootsHealth's vitamin D testing kit and learn more about vitamin D and its impact on your health. from http://articles.mercola.com/sites/articles/archive/2020/09/23/coronavirus-2nd-wave.aspx The Health and Human Services' Operation Warp Speed pledges to deliver 300 million doses of a COVID-19 vaccine by 2021.1 However, developing a safe and effective vaccine normally takes years and begins with animal studies. Given the urgency of the COVID-19 pandemic, vaccine makers are rushing into human clinical tests and circumventing lengthy animal trials. Such fast-tracked vaccines pose unknown risks to humans, which are magnified because governments are granting COVID-19 vaccine makers immunity from liability for all vaccine injuries and deaths that occur after the vaccines are recommended (or mandated) by public health officials.2 In August, AstraZeneca announced that most countries it expects to supply with COVID-19 vaccine will grant the pharmaceutical company liability protection when people are harmed by the new vaccine. In the U.S., vaccine makers already have something of a "free pass" when it comes to vaccine injury liability and lawsuits through the National Childhood Vaccine Injury Act of 19863 and the Public Readiness and Emergency Preparedness (PREP) Act, passed in 2005 (more on those later.)4 The main concern is that the combination of COVID-19 vaccines being fast-tracked to market at "warp speed" with minimal testing, together with blanket liability protection for Pharma for injuries their products cause, is a public health nightmare waiting to happen. Vaccine Makers Already Enjoy Protection in the USWhen the National Childhood Vaccine Injury Act became law in 1986, it gave vaccine manufacturers partial liability protection from lawsuits and did not protect doctors or other vaccine providers for vaccine injury malpractice claims. The 1986 Act established a federal no-fault vaccine injury compensation program (VICP) as an administrative alternative to a lawsuit for injuries caused by vaccines recommended by the CDC for children. Contested vaccine injury claims are adjudicated by U.S. Court of Federal Claims in Washington, D.C., and there is a Trust Fund out of which claims are paid, sparing insurance companies representing vaccine makers and vaccine providers from costly payouts for vaccine injuries and deaths.5 According to Legal Talk Network, the purpose for the 1986 Act was to induce vaccine makers wary of costly vaccine injury lawsuits to stay in the vaccine manufacturing business and create and market vaccines with impunity and no fear of being sued.6 Unfortunately, the bottom line is that, today, if you receive an FDA-licensed and state-mandated vaccine that injures or kills you or your child, the vaccine maker and the health care practitioner who administered the vaccine are protected from being sued in civil court. But the story behind it goes far deeper. The Act Admits That Vaccines Can and Do Cause Injury, DeathBarbara Loe Fisher, co-founder and president of the National Vaccine Information Center, worked closely with Congress7 for years before the 1986 Act became law. In the historic federal legislation that was characterized by the pharmaceutical and medical care industries as badly needed "tort reform," the U.S. government acknowledged for the first time that:8 1. Federally licensed and recommended vaccines mandated by states for children to attend school can and do cause injury and death 2. Vaccine safety should be a priority for health agencies, vaccine manufacturers, doctors and other vaccine administrators 3. Individuals injured by government recommended and mandated childhood vaccines should have access to a federal vaccine injury compensation program administrative alternative to filing a vaccine injury lawsuit in civil court. Furthermore, they should have access to the civil court system in cases where: • Federal compensation is denied or is inadequate • There is evidence a pediatrician or other vaccine administrator negligently administered a vaccine • A vaccine manufacturer engaged in criminal fraud or negligence • A vaccine manufacturer could have made a vaccine less harmful (design defect) New Laws and Rulings Chip Away at the ActAccording to NVIC, the safety and compensation provisions in the 1986 law have been chipped away to the point that the law has been fatally compromised. At the time the Act was passed:9
The erosion of the law continued in 2011 when, in a split decision, the U.S. Supreme Court:
According to NVIC:13
With No Liability Vaccine Makers Race to Make VaccinesWith the threat of vaccine injury lawsuits removed, more pharmaceutical companies have entered the lucrative vaccine business. For the past three decades, the global vaccine industry has been busy creating hundreds of new experimental vaccines, pushing for some of them to be fast-tracked, even before the recent push for a COVID-19 vaccine. It doesn't matter how sloppy their work is or whether there is a lack of safety testing because, with no liability, there is no reason for safety testing, Robert Kennedy Jr., founder and chairman of the board of directors of the Children's Health Defense, says in a video.14 Their biggest cost, "paying liability at the back end," is not there, Kennedy says. "There's no reason to make [vaccines] safe because nobody can sue [them] … there's no consequence of giving you a really dangerous vaccine … it's a goldmine. If you can get a vaccine on the CDC schedule, it's worth a billion dollars a year typically to your company." Moreover, the public has no redress against potential harm from the vaccine companies. "You cannot sue them for redress," says Kennedy. "There's no discovery; there's no depositions; there's no medical malpractice; there's no class actions." The PREP Act Also Protects Vaccine MakersIn 2005, the Public Readiness and Emergency Preparedness Act (PREP Act) was passed as part of Bioshield legislation addressing potential bioterrorism threats after 9/11. The PREP Act shields vaccine makers from lawsuits for injuries caused by vaccines created and used during a declared public health emergency (such as the COVID-19 pandemic). According to the Department of Health and Human Services, the PREP Act provides immunity from "claims of loss caused" by countermeasures or treatment of:15
Like the National Childhood Vaccine Injury Act, the Public Readiness and Emergency Preparedness Act of 2005, or Prep Act, facilitates the administration of potentially inadequately tested, risky vaccines and drugs by releasing drug manufacturers from all liability for covered "countermeasures." Moreover, it gives the Secretary of HHS the power to detain, examine and quarantine indefinitely any individual thought to be infected with a communicable disease. When the Act was passed in 2005, it paved the way for then HHS Sec. Kathleen Sebelius to impose quarantines and mandatory vaccinations if deemed necessary for the swine flu pandemic occurring at the time. Today, of course, the PREP Act allows those same scenarios as they relate to the COVID-19 pandemic. AstraZeneca: Fast-Tracked Vaccines Need Liability ShieldMarketing of a COVID-19 vaccine is developing rapidly, especially in the U.K., where the government has signed vaccine supply pacts with AstraZeneca and Oxford, Pfizer, BioNTech, Valneva, Sanofi and GlaxoSmithKline.16 Yet, a recent article in Stat News asked "would vaccine manufacturers be willing to roll out vaccines on such a slight evidence base" without a liability shield? It's a good question that the article really didn't answer.17 Experts admit that "fast-tracking" to licensure an experimental vaccine like COVID-19 at "warp-speed" has never been done and is problematical for public safety. In an interview with Harvard Business School, Ken Frazier, chairman and CEO of Merck & Co., said:18
Officials at AstraZeneca, the U.K.'s second-largest drug maker, acknowledge that the risks of a hastily-marketed and tested vaccine necessitate a shield from risk which they have sought.
A Grave Risk Barely Acknowledged by Big VaxThe history of vaccines against coronaviruses has not been encouraging — a paradoxical effect has been seen. Rather than fighting the infection, they can actually trigger what's known as paradoxical immune enhancement. What this means is that, despite a robust antibody response when you're exposed to the actual virus, rather than protecting you, the vaccine actually enhances the virus' ability to make you sick or even kill you. This paradoxical effect means that "the most hazardous hurdle for the inoculation is … challenging participants with wild COVID infection," says Kennedy.20 "Past attempts at developing COVID vaccines have always faltered at this stage as both humans and animals achieved robust antibody response, then sickened and died when exposed to the wild virus." He gives a chilling example:
Research published in the Journal of Translational Autoimmunity confirms that treatment with a vaccine may increase the risks associated with a wild type virus rather than protect against it. The researchers call the process pathogenic priming.21
The pathogenic priming is consistent with other autoimmunity actions including the release of proinflammatory cytokines creating a storm, states the research. It has been seen in coronaviruses similar to COVID-19:22
Why would the recombinant vaccines create a greater risk for wild type viruses rather than protect against them? Because, according to the research, immunogenic peptides in viruses have "high local homologous matching"23 to human proteins, meaning they closely resemble each other allowing opportunistic invasion. The immunogenic peptides have:24
The research concludes that such similarity between viruses and human proteins, called homology, likely explains the previous failure of SARS and MERS vaccines in the past and dooms a COVID-19 vaccine as well. New COVID-19 Vaccine Technology Has Not Been Used BeforeThere is another risk with at least one of the new COVID-19 vaccine candidates, which uses a type of technology never before used in human vaccines, called mRNA. According to Dr. Andrew Kaufman, a forensic psychiatrist who formerly served as clinical assistant professor of psychiatry at SUNY Upstate Medical University,25 RNA vaccines actually change the genetic makeup of our own cells in a form of gene therapy.26 While news outlets claim to have debunked27 Kaufman's evaluation, the fact remains that this is a type of vaccine that has never been licensed for use in humans before — so how do the debunkers know for certain that it doesn't change your DNA? Conventional vaccines train your body to recognize and respond to the proteins of a particular virus by injecting a small amount of the actual viral protein into your body, thereby triggering an immune response and the development of antibodies. But, mRNA vaccines are designed to co-opt your body to force it to produce its own viral protein, which, theoretically your immune system should then attack. As I said, the danger is that no previous vaccines have had your own cells produce the viral proteins responsible for producing immunity and no one can predict what will happen, especially for individuals genetically and epigenetically predisposed to developing autoimmune disorders. What might go wrong when you turn your body into a viral protein factory making antibodies on a continual basis? Again, no one knows since no mRNA vaccines are on the market and their first users will be guinea pigs. But, according to researchers at the University of Pennsylvania and Duke University.28
When looking at other research the scientists also worried about blood clots and edema, and some of these effects, such as systemic inflammation and blood clots, resemble severe symptoms of COVID-19 itself. Since the changes work at the genetic level, could this vaccine technology create long-term or even generational effects in the human genome? Brave New Vaccine TechnologyTo repeat, mRNA technology has never been approved for use in human vaccines that will function very differently from traditional vaccines. The mRNA technology is not like other viruses where a vaccine is inactivated or simply weakened. In a video Kaufman says:29
The electrodes generate an electric current inside of our cells called electroporation:
The bottom line is, Kaufman says, not only is the source of the genetic material found in the vaccine undetermined, but the brave new vaccines could be used for "all sorts of purposes that we may not know about."30 Extending protection from liability to vaccine-makers allows the irresponsible sale and marketing of vaccines that have been poorly tested and formulated because the manufacturers have "nothing to lose." If the mRNA vaccine technology found in many COVID-19 vaccines harms us and permanently alters our genes, unaccountable vaccine manufacturers will be totally off the hook. from http://articles.mercola.com/sites/articles/archive/2020/09/22/warp-speed-vaccine-will-be-shielded-from-liability.aspx As the National Vaccine Information Center (NVIC) prepares to host the three-day, three-night Fifth International Public Conference on Vaccination that will be broadcast online October 16 through 18, 2020, the theme we have chosen is “Protecting Health and Autonomy in the 21st Century,” because at no time in modern history has it been more important for all of us to take a stand and do just that. This year, the orchestrated actions by governments around the world to restrict or eliminate civil liberties in response to the emergence of a new coronavirus has been unprecedented, and has had profound effects on the global economy and on the physical, mental and emotional health of billions of people.1 By mid-September 2020, there were about 29 million cases of the new Severe Acute Respiratory Syndrome (SARS-CoV-2) reported worldwide with about 925,000 associated deaths. The United States, the third most populated country in the world at 330 million people, had recorded over 7 million cases and 198,000 deaths, with an estimated 598 deaths per million people, which is a higher death rate per million people than Sweden,2 where health officials have refused to order masking or lock down the country and allowed the population to acquire natural herd immunity to the virus.3,4 Overall COVID-19 Mortality Is Less Than 1%According to the World Health Organization, the overall infection mortality rate for the new SARS coronavirus causing COVID-19 is about 0.6%,5 although some scientists say it is lower,6 while others estimate it can be as high as 1 to 2% in some parts of the world.7 Compared to Ebola with a 50% mortality rate8 or smallpox that killed 30%,9 or tuberculosis that still is a deadly disease killing 20% to 70%,10 or diphtheria at 5% to 10%,11 or the 1918 influenza pandemic with a 2.5% mortality rate,12 COVID-19 is near the bottom of the infectious diseases mortality scale with a less than 1% mortality rate in most countries. Those at highest risk for complications and death include the elderly and those with one or more poor health conditions.13 The CDC recently reported that only 6% of COVID-19-related deaths were solely due to coronavirus infection and 94% of the people who died also had influenza or pneumonia; heart, lung or kidney disease; high blood pressure; diabetes, or another underlying poor health condition.14 Most studies suggest it is rare for children to suffer complications and die from COVID-19.15 But seven months after the World Health Organization (WHO)16 declared a coronavirus pandemic,17 and public health officials persuaded lawmakers to turn the world upside down, a lot of people are asking questions and so are doctors who disagree with each other about the facts. Questions like: Where did the new respiratory virus come from? The most popular narratives about the mutated coronavirus is that it either jumped out of a bat or another animal in a Chinese wet food market18,19 or escaped out of a biohazard lab in 2019,20,21 but scientists continue to argue about which scenario is more likely.22 And this question: If I wear a cloth facemask, does it really prevent me from getting infected with or transmitting COVID-19? There is an ongoing debate in the medical community about whether it is a good idea for all healthy children and adults to wear cloth masks when they leave their home.23 In March 2020, the U.S. Surgeon General ordered the American public to stop buying and wearing masks because “they are not effective in preventing general public from catching coronavirus”24 and “actually can increase the spread of coronavirus," which was the position of the World Health Organization.25 But in April, the CDC walked back its “do not mask” order and urged all healthy Americans to voluntarily wear homemade cloth face coverings when entering public spaces.26 In June, the WHO was continuing to say that, “At the present time, the widespread use of masks everywhere is not supported by high-quality scientific evidence, and there are potential benefits and harms to consider … Masks on their own will not protect you from COVID-19.”27 But by June, a number of state Governors and local governments had mandated facemask wearing and an epidemic of mask shaming had begun,28,29 which led to public protests against masking mandates.30 In August, the CDC doubled down and expanded face masking directives to include all children over the age of 2,31 while the WHO warned that children under the age of 6 should not wear masks but children over age 12 should.32 So, confusion reigns. While some scientists are saying that if all healthy people are forced to wear face masks it will not stop the coronavirus pandemic and gives a dangerous and false illusion of safety,33 other scientists are demonizing the refusers, alleging that people refusing to mask up are “sociopathic” and have lower levels of empathy.34 About 30 U.S. states require masking for young children and adults who enter public spaces,35 and some states are leveling steep fines of up to $1,000 or threatening jail time for anyone who fails to comply.36 Washington state has made not wearing a mask in public a misdemeanor crime37 and central Texas officials say they wish they could put people in prison for refusing to wear a mask.38 More than 50 countries in the world now require people to cover their faces when they leave home and some do fine and imprison people who go outside without wearing a mask.39 So, what about getting tested for COVID-19? The CDC says that people should get tested if they have COVID-19 symptoms or have been in contact with someone who has been diagnosed with the infection. There is also an antibody test to identify whether or not you have been infected in the past.40 But lab tests are not always reliable and people are asking this logical question: If I get a lab test, will it accurately identify if I am currently infected or have been infected with COVID-19 in the past? Unfortunately, it’s not clear how accurate any of the tests are, especially the antibody test for past infection because the presence of antibodies may not be the only way to measure immunity.41 The best guess is that the range of reported false negative results for the nasal swab test is between 2% and 50%, and the reported false negative results for the antibody blood test is up to 30%, depending upon when during or after the infection testing is performed.42 In July, a state lab in Connecticut admitted that 90 out of 144 people tested during a 30-day period — most of them nursing home residents — were inaccurately informed they were infected because of faulty, false positive lab tests.43 In August, 77 football players in the National Football League were given false positive test results when, after retesting, all the tests came back negative.44 People are also wondering what happens after they get COVID-19, asking this question: If I recover from COVID-19 will I only get temporary immunity or will I have long-term immunity against reinfection? The CDC says it is unknown how long immunity lasts or whether you can get the new coronavirus infection twice.45 However, last spring researchers found that out of 68 uninfected persons, the blood from one third of them contained helper T-cells that recognized the mutated SARS coronavirus. They concluded the presence of these defensive helper T cells gives evidence for some residual immunity that may have been produced after common cold infections caused by other types of coronaviruses. This, the scientists said, “bodes well for the development of long-term protective immunity.”46 Another important study was published in the medical literature in August providing evidence for robust memory T cell immune responses in people who had recovered from even mild or asymptomatic cases of COVID-19, but had no detectable virus-specific antibodies.47 If people can have strong immune responses without symptoms and traditional antibody tests for proof of immunity don’t apply to COVID-19, public health officials may be underestimating the extent of population-level herd immunity that already exists in the U.S., where there have been more cases reported than anywhere else. COVID-19 Public Health Laws a Public Relations DisasterWhile doctors debate the science, it is becoming clearer that the response to the new coronavirus infection by government health officials has been a public relations disaster. The anxiety, fear and chaos created by regulations instituted by most governments after the declaration of a COVID-19 pandemic this year has torn the fabric of societies and affected public opinion about public health laws and vaccination.48 Now the people are being told that there is one — and only one — simple solution to resolving the crisis and getting back to normal: that is, the only way we can take off our masks and touch, hug, kiss or come close to each other again49,50,51,52,53,54 is for every person living in every country to get injected with one of the liability-free COVID-19 vaccines being fast tracked to market.55,56,57,58,59 In April, WHO officials at the United Nations launched a global initiative “to end the COVID-19 pandemic,” proclaiming that “no one is safe until everyone is safe.”60 By May, they were warning that if every person in the world doesn’t get injected with a COVID-19 vaccination, the virus “may never go away.”61 The WHO,62 U.S. government63,64,65,66 and lawmakers in the European Union,67 along with wealthy and politically powerful nongovernmental organizations (NGOs) like the Gates Foundation,68,69,70 GAVI, the Vaccine Alliance,71 and Coalition for Epidemic Preparedness Innovations (CEPI)72 have given the pharmaceutical industry tens of billions of dollars to develop and fast-track experimental coronavirus vaccines to market and promote their universal use.73,74 At the same time, governments have given pharmaceutical companies a liability shield from lawsuits when COVID-19 vaccines injure or kill people.75,76 The hard sell is on, but a lot of people are NOT buying it. People Are Rejecting the COVID-19 Vaccine Sales PitchEvery poll taken this year has revealed that between 40% and 70% of people living in the U.S. and Europe do not plan to get a COVID-19 vaccine when it is licensed.77,78,79,80,81,82 Populations in developed countries are resisting the siren call for “solidarity,” as doubt about COVID-19 vaccines is becoming more common in developing counties, too.83 The pushback by a wary public has taken government officials by surprise. Apparently, they were banking that the economic and social deprivation, fear and chaos surrounding lockdowns would produce a bull market for experimental mRNA and DNA COVID-19 vaccines using technology that never has been licensed for humans.84 It is widely acknowledged now that a solid two-thirds of Americans or more will “just say no” to getting injected with a vaccine containing lab altered parts of a new coronavirus that scientists admit they still don’t know much about,85 vaccines that preliminary clinical trials have revealed may well cause more than just a few minor reactions.86 A frustrated top U.S. health official has name-called Americans who refuse to go along with public health policies and laws, calling them “anti-science” and “anti-authority.”87,88 The truth is, people in this country and many others just don’t have confidence in the quality and quantity of the science or government health officials they are being told to trust.89 Angry that a growing number of people are reluctant to roll up their sleeves for a vaccine that is being rushed to market at “warp speed,” public health officials,90 billionaire Silicon Valley technocrats,91,92,93 doctors, attorneys and bioethics professors94,95,96,97,98 and politicians99 are beating the drum for swift enactment of “no exceptions” mandatory vaccination laws as soon as COVID-19 vaccines are licensed.100 Already, some cheerleaders at leading universities are banging that drum for approving and using experimental COVID-19 vaccines even before testing is done,101 and are calling for young, healthy people to be the first to get the vaccine because it is their “civic duty” to protect everyone else.102 They warn that “herd immunity may not be achieved if people refuse to take the coronavirus vaccine,”103,104 and say that, in order to keep society “safe,” laws must be passed to threaten and coerce you and your minor children to get vaccinated or face crippling social sanctions that will effectively take away your liberty and destroy your life.105 People in US and Other Nations Rise to Defend FreedomThis summer, huge public demonstrations defending freedom in Berlin,106 London,107 Paris108 and Copenhagen saw tens of thousands of citizens gather to protest masking109 and other oppressive coronavirus lockdown policies, which have severely restricted normal physical contact between people, caused widespread unemployment,110 and harmed their physical, mental and emotional health.111 Like in Europe, people living in Canada,112 Australia113,114 and New Zealand115 also are resisting months of social distancing policies that have eliminated fundamental human rights, such as freedom of speech and assembly. The U.S. has seen similar but smaller public demonstrations opposing forced masking, social distancing and lockdown laws and defending freedom in Virginia,116 Pennsylvania,117 Wisconsin,118 Michigan,119 California120 and other states, as record numbers of Americans struggle with unemployment,121,122 the destruction of small middle class businesses,123 mortgage defaults124 and bankruptcy filings;125 steep increases in anxiety and depression,126,127 drug and alcohol addiction,128 child and spousal abuse,129 and divorce.130 Social Sanctions for Failure to Get Vaccinated May Align With Lockdown SanctionsThe punishing social sanctions being talked about if you refuse a COVID-19 vaccination are likely to be enforced using government-operated electronic tracking systems linked to digital “immunity passports” that require you to “prove” you are immune to the new SARS coronavirus before you are allowed to work in an office building or enter other public spaces.131,132,133,134 These social sanctions for failure to vaccinate may closely resemble the types of social interaction restrictions enforced in the U.S. and other countries over the past year. In the U.S., most public health laws, including vaccine laws, are enacted by the states,135 while the federal government makes vaccine use recommendations and can mandate vaccines for people crossing national or state borders. Local city and county governments also can impose their own public health regulations.136 That is why some states and cities have seen very restrictive COVID-19 pandemic masking137 and lockdown regulations138 and others have been more open.139 So, whether or not you will be punished for refusing to get a COVID-19 shot next year primarily will be determined by your state’s governor and the representatives who have been elected to make laws in your state capitol.140 Depending upon where you live and the political philosophy of the majority of representatives in your state legislature, after the COVID-19 vaccine is licensed by the federal Food and Drug Administration (FDA) and recommended by the CDC for use by all children and adults,141 if you refuse to get a COVID-19 shot, you could be blocked from:142
And you could be prohibited from checking into a hospital for surgery, or visiting a family member in a nursing home, or blocked from obtaining private health insurance and Medicaid or Medicare. In other words, if you refuse to get a coronavirus vaccination, you could be subjected to the kinds of punitive social sanctions I have been predicting and publicly warned about since 1997,143,144,145,146 sanctions that are already being applied to Americans who decline to get or give their children dozens of doses of CDC “recommended” liability-free vaccines147 and already are being denied an education, medical care and employment.148,149 Broken Promises Leads to Broken TrustDoctors and public health officials wondering why people don’t trust what they say about infectious diseases and vaccination, including coronavirus and COVID-19 vaccines, only have to look in the mirror to answer the question. Since 1982, parents of vaccine injured children have been begging doctors to do the kind of science that will explain why so many highly-vaccinated children, who don’t get measles or chicken pox anymore, are stuck on sick and suffering with brain and autoimmune disorders that never go away.150 For four decades, we have been asking doctors and government health officials to stop sweeping casualties of inhumane one-size-fits all vaccine policies, under the rug.151 What we get from medical professors in universities receiving lots of money from the government and pharmaceutical companies, and from doctors developing vaccines, and from public health officials pushing “no exceptions” vaccination policies are threats, name-calling, bullying and punishment if we try to exercise informed consent to vaccination.152,153,154 There is no other word for it but abuse. They order us to obey them but refuse to take responsibility for what happens when we obey the orders they give. They expect us to trust them and refuse to care about the victims of vaccination when the benefits do not outweigh the risks. Instead, they act to protect the power and profit-making of their business partners: the pharmaceutical industry, medical trade associations, multinational media corporations and Silicon Valley billionaires, and leave vaccine victims to take care of themselves. What’s trust got to do with it? Broken trust has everything to do with why the majority of people in the U.S. and Europe do not want to roll the dice and find out whether the odds of surviving a COVID-19 vaccination are in their favor. It is during this extraordinary time of great challenge and opportunity that NVIC is sponsoring the Fifth International Public Conference on Vaccination. Our conference will create an expanded base of knowledge about vaccine science, policy, law and ethics brought to you by more than 40 distinguished speakers, who will empower you with information you need to become an effective vaccine freedom advocate. Go to NVIC.org and register today for this historic conference celebrating freedom of thought, speech and conscience and gain permanent online access to this valuable video library of information. It’s your health, your family, your choice. And our mission continues: No forced vaccination, not in America. from http://articles.mercola.com/sites/articles/archive/2020/09/22/coronavirus-vaccine-news.aspx The U.S. Health and Human Services' Operation Warp Speed has pledged to deliver 300 million doses of a COVID-19 vaccine by 2021,1 if not sooner.2 However, developing a safe and effective vaccine normally takes years and begins with animal studies. The COVID-19 vaccines are all being rushed straight into human clinical tests, forgoing lengthy animal trials altogether. Such fast-tracked vaccines pose unknown risks, which are further magnified since governments are granting COVID-19 vaccine makers immunity from liability for all vaccine injuries and deaths that occur after the vaccines are recommended (or mandated) by public health officials.3 At the end of July 2020, AstraZeneca announced4 most countries it expects to supply with COVID-19 vaccine will grant the pharmaceutical company complete liability protection if people are harmed. In the U.S., vaccine makers already have something of a "free pass" when it comes to vaccine injury liability and lawsuits through the National Childhood Vaccine Injury Act of 19865 and the Public Readiness and Emergency Preparedness (PREP) Act, passed in 2005.6 The main concern is that the combination of COVID-19 vaccines being fast-tracked to market at "warp speed" with minimal testing, together with blanket liability protection against vaccine injuries could be a public health nightmare in the making. Problems With Moderna’s Vaccine Are Becoming ApparentEarly warning signs that something might be amiss have already started emerging. As detailed in “Gates Tries to Justify Side Effects of Fast-Tracked Vaccine,” results7 from Moderna’s Phase 1 human trial revealed 100% of volunteers in the high-dose group suffered systemic side effects. Side effects included fatigue, chills, headache and myalgia (muscle pain); 21% suffered “one or more severe events.” According to Bill Gates, those side effects are largely due to the high dosages Moderna had to use in order to achieve desired antibody levels. But, if high dosages are required to create a robust-enough immune response, and higher dosages also cause systemic side effects in nearly all people, just how safe will this vaccination campaign be? In July, it was reported8 that the 100-mcg dose vaccine — despite its 100% side effect ratio after the second dose — would proceed to Phase 3 trial assessment. In a May 26, 2020, article9 in STAT news, Ian Haydon, one of the Phase 1 study participants who suffered severe side effects requiring hospitalization, stated that while he recovered, the inoculation left him feeling “as sick as he’d ever felt.” As noted by Robert F. Kennedy Jr.:10
Moderna Patent ProblemsOther signs of trouble include reports that Moderna has no legal rights to a key patent for its vaccine delivery system, and that company executives are now dumping their stocks. There are also questions emerging as to whether Moderna had some sort of foreknowledge that a coronavirus pandemic might be in the making. In the video above, independent journalist Ben Swann reports Moderna filed a patent amendment in March 2019, nine months before the COVID-19 pandemic started, stating there was a need for this vaccine technology out of concern for “reemergence or deliberate release of the SARS coronavirus.” The amendment was done to a patent application that had been repeatedly rejected since its initial filing in 2015. The March 2019 amendment stressed the importance of obtaining this patent due to concerns of a beta coronavirus pandemic. Of all the viruses in the world, why would they suspect a coronavirus pandemic? In December 2019, the U.S. Patent Office issued a final rejection of Moderna’s patent application, yet when the COVID-19 pandemic broke out in early 2020, Moderna was among the first to state they had the ability to address the problem. It wasn’t until May 2020, months after it had already entered into partnership with the U.S. National Institutes of Health to develop the vaccine, that Moderna was finally issued the patent for it. And, even then, a key patent for the technology already belonged to another company. The NIH also holds many patents on the core mRNA technology used by Moderna. David E. Martin, Ph.D., a national intelligence analyst featured in Swann’s video report, points out that even though Moderna “very clearly did not have the legal right, and they did not have the contractual rights, they didn’t have the licensing rights” required to enter into a federal contract, they were still somehow pushed to the front of the line by the NIH and Dr. Anthony Fauci.
Martin goes on to explain how both Moderna and the NIH are essentially engaged in patent infringement, as a core part of the technology — the lipid nanoparticle technology that is part of the vaccine delivery system — belongs to another company. Moderna sought to invalidate the patent owned by Arbutus Biopharma, but lost the challenge at the end of July 2020.11,12 As a result, Arbutus might be able to make a royalty claim in the vaccine, and news of the failed patent challenge caused Moderna’s stock to drop by 9.5%.13 Moderna Executives Have Raked in Millions on Dumped StocksAs reported by NPR14 September 4, 2020, executives at Moderna have also cashed in stock options, raking in tens of millions of dollars of personal profit in the process. Considering the patent problems now emerging and the lingering safety and efficacy questions, this move has raised significant concerns among financial experts:
Importantly, NPR discovered that several of the executives appear to have made “questionable modifications to stock sale plans” shortly before key announcements were made about the vaccine — in some cases just a single day ahead of the announcements. In order to be legal, prescheduled stock sale plans must be made at a time when no confidential inside information is available that may influence their sales decisions, so the timing of their modifications appears suspicious. What’s more, as a general rule, corporate best practices call for leadership to maintain stock in the company to ensure they have sufficient incentive to improve company performance. Two Moderna executives, however, have sold all of their stock holdings, and its general counsel has sold “nearly all” of hers, NPR reports.15 What Do Moderna Execs Know That We Don’t?Why would executives unload their stocks before the vaccine is even launched? Do they suspect or know something has, or is about to go awry? As of right now, there’s no evidence whatsoever that the company’s novel vaccine will actually work, let alone be safe. According to NPR:16
Coronavirus Vaccines Have Never Been Successfully MadeAs I’ve discussed in several previous articles, COVID-19 vaccine manufacturers have several hurdles to overcome, as coronavirus vaccine development has been notoriously challenging. In the 20 years that vaccine makers have tried to develop a coronavirus vaccine, efforts have failed due to dangerous, many times lethal, side effects. Adding to the problem is that many of them are relying on novel mRNA technology that has never been used in vaccines before.17 Making matters even worse, the vaccines are not safety tested against inert placebo, as is the gold standard for drug safety research. Oxford University’s mRNA vaccine, ChAdOx1 nCoV-19, for example, is being compared to a meningitis vaccine.18 As discussed in “Dangerous Placebos Used in Medical Trials,” using an active substance such as another vaccine destroys any hope of a valid safety study. This is just one way in which vaccine makers cheat in their safety studies to minimize the appearance of adverse effects. In the case of a COVID-19 vaccine, establishing safety is of utmost importance, as previous coronavirus vaccines have caused paradoxical immune enhancement — a situation in which the vaccine actually makes you more susceptible to severe illness and death once you’re infected with the actual virus. Kennedy explained this in my interview with him, featured in “Robert F. Kennedy Jr. Explains Well-Known Hazards of Coronavirus Vaccines.” A short clip of that interview is included below. Aside from the possibility of a paradoxical immune response, mRNA vaccines may in and of themselves be problematic. According to researchers at the University of Pennsylvania and Duke University:19,20
AstraZeneca Stopped Its Vaccine Trial Due to Side EffectsSeptember 8, 2020, STAT News reported21 that AstraZeneca has temporarily halted its Phase 3 vaccine trials due to “a suspected serious and unexpected adverse reaction” in a British participant. The company did not divulge the nature of the adverse reaction. The New York Times claims22 “a person familiar with the situation, and who spoke on the condition of anonymity” said the individual ”had been found to have transverse myelitis, an inflammatory syndrome that affects the spinal cord and is often sparked by viral infections.” AstraZeneca, in collaboration with the University of Oxford, is conducting Phase 2/3 trials for their mRNA COVID-19 vaccine (ChAdOx1 nCoV-19, a chimpanzee adenovirus modified to carry and deliver coronavirus genes into human cells) in the U.K. and India, as well as Phase 3 trials in Brazil, South Africa and the U.S.23 According to STAT News:24
AstraZeneca Vaccine Has High Rates of Side Effects TooLike the Moderna vaccine, the AstraZeneca/Oxford University vaccine also appears to come with a shockingly high rate of side effects. Results25 from one of its Phase 1/2 studies published August 15, 2020, revealed a clear majority of participants experienced side effects. Results showed:26
Prepare by Attending NVIC Online Conference in OctoberIf you’re concerned about the possibility of COVID-19 vaccine mandates, be sure to attend the Fifth International Public Conference on Vaccination sponsored by the National Vaccine Information Center (NVIC) — an online event held October 16 through 18, 2020. This year’s theme is “Protecting Health and Autonomy in the 21st Century.” The conference will bring together well-known speakers from around the world — including yours truly — who will present information on vaccine science, policy, law, ethics and civil liberties and will feature formal presentations, panel discussions and live chat rooms. NVIC has held four previous hotel-based conferences in the Washington, D.C., area but, this time around, the conference will be held online due to the unpredictability of government regulations related to COVID-19, including travel and social distancing restrictions that may still be in play in October. 
Also, sign up for the NVIC Advocacy Portal. It’s a free service that will keep you informed and up-to-date about proposed vaccine-related legislation happening in your state that could further restrict or eliminate your legal right to make voluntary vaccine decisions for yourself and your children. from http://articles.mercola.com/sites/articles/archive/2020/09/21/coronavirus-vaccine-patent.aspx |
Nia Pure NatureThe Provider of premium Quality Health Products To Live Better Lives Archives
March 2022
Categories |
 RSS Feed
RSS Feed
