|
Fibromyalgia, characterized by chronic, widespread pain is an often-debilitating condition that primarily affects women. While as many as 10 million Americans have fibromyalgia, its cause remains a mystery. Brain scans of fibromyalgia patients have offered hard evidence that the pain they experience is indeed real — mainly because their threshold for tolerating pain impulses is substantially lower than that of most individuals. But the mechanism causing this lowered pain threshold is still unknown. Some experts, such as Dr. Frederick Wolfe, the director of the National Databank for Rheumatic Diseases and the lead author of the 1990 paper that first defined fibromyalgia's diagnostic guidelines, believe fibromyalgia is mainly a physical response to mental and emotional stress. But while stress and emotions may indeed play an important role, more recent research shows fibromyalgia patients tend to have severe inflammation in their body, including their nervous system and brain. Signs and Symptoms of FibromyalgiaDiagnosis can be a challenge, but the updated case definitions of fibromyalgia, issued in 2010 and later simplified in 2012, claim to correctly diagnose about 83 percent of cases.1 Originally, the condition was thought to be a peripheral musculoskeletal disease. Today, fibromyalgia has become increasingly recognized as a neurobiological problem causing central pain sensitization. Unfortunately, there are currently no laboratory tests available for diagnosing fibromyalgia, so physicians primarily depend on patient histories, reported symptoms and physical exam findings. Classic symptoms of this condition include: • Pain — The key marker of fibromyalgia is pain, which is profound, widespread and chronic. Pain inside of your elbows and knees, collarbones and hips is indicative of fibromyalgia when it's present on both sides. People also frequently report pain all over their bodies — including in their muscles, ligaments and tendons — and the pain tends to vary in intensity. It has been described as deep muscular aching, stabbing, shooting, throbbing and twitching. Neurological complaints add to the discomfort, such as numbness, tingling and burning. The severity of the pain and stiffness is often worse in the morning. Aggravating factors include cold/humid weather, nonrestorative sleep, fatigue, excessive physical activity, physical inactivity, anxiety and stress. • Cognitive impairment — So-called "fibro-fog" or foggy-headedness is a common complaint. • Fatigue — The fatigue of fibromyalgia is different from the fatigue that many people complain of in today's busy world. It is more than being tired; it's an all-encompassing exhaustion that interferes with even the simplest daily activities, often leaving the patient with a limited ability to function both mentally and physically for an extended period of time. • Sleep disruption — Another major part of the diagnostic criteria for this condition is some type of significant sleep disturbance. In fact, part of an effective treatment program is to make sure you're sleeping better. Medical researchers have documented specific and distinctive abnormalities in the Stage 4 deep sleep of fibromyalgia patients. During sleep, they are constantly interrupted by bursts of awake-like brain activity, limiting the amount of time they spend in deep sleep. • Other symptoms — Other common symptoms include irritable bowel and bladder, headaches and migraines, restless leg syndrome and periodic limb movements, impaired memory and concentration, skin sensitivities and rashes, dry eyes and mouth, anxiety, depression, ringing in the ears, dizziness, Raynaud's Syndrome and impaired coordination. Conventional treatment typically involves some form of pain medication, and perhaps psychotropic drugs like antidepressants. I don't recommend either as they fail to address the cause of your problem. Many fibromyalgia sufferers also do not respond to conventional painkillers, which can set in motion a vicious circle of overmedicating on these dangerous drugs. Brain Inflammation — Another Hallmark of FibromyalgiaUsing PET imaging, a recent investigation2 by researchers at Massachusetts General Hospital and Karolinska Institutet in Sweden revealed the presence of widespread brain inflammation in patients diagnosed with fibromyalgia.3,4 Earlier research5 conducted at Karolinska Institutet also discovered high concentrations of cytokines (inflammatory proteins) in the cerebrospinal fluid, suggesting fibromyalgia patients have inflammation in their nervous system as well.6 The team at Massachusetts General Hospital, meanwhile, has previously shown that neural inflammation, and glial cell (immune cells) activation specifically, plays a role in chronic back pain. Animal studies have also offered evidence for the hypothesis that glial cell activation can be a cause of chronic pain in general.7 Here, they found that when glial cells in the cerebral cortex were activated, the more aggressive the activation, the greater the fatigue experienced by the patient. As reported by Medical Life Sciences:8
Brain Inflammation Linked to Loss of Brain CellsIn related news, German researchers investigating inflammation mechanisms in the brain have found that as mice get older and regulation of inflammatory responses become increasingly impaired, they start losing brain cells.9 Interestingly, the cannabinoid receptor type 1 (CB1), which produces the "high" in response to tetrahydrocannabinol (THC) in marijuana, also helps regulate inflammatory reactions in your brain. In short, chronic brain inflammation is in part driven by the CB1 receptors' failure to respond. To understand how this works, you need to know a little bit about how microglial cells work. Microglial cells are specialized immune cells found in your central nervous system, including your spinal cord and brain. These immune cells respond to bacteria and are responsible for clearing out malfunctioning nerve cells. They also signal and recruit other immune cells when needed and trigger the inflammatory response when necessary. Problems arise when the inflammatory response becomes dysregulated and overactive. In the brain, the inflammation can easily damage healthy brain tissue. The "brake signal" that instructs glial cells to stop their inflammatory activity is endocannabinoids, and the endocannabinoids work by binding to certain receptors, including CB1 and cannabinoid receptor type 2 (CB2). Immune Cells Communicate and Influence Inflammatory Response Using EndocannabinoidsCuriously, microglial cells have virtually no CB1 and very few CB2 receptors, yet they still react to endocannabinoids. The present study was designed to investigate this puzzling riddle. As it turns out, there's a type of neuron that does contain a large number of CB1 receptors, and it appears that it is the CB1 receptors on these specific neurons that control microglial cell activity. In other words, it appears microglial cells do not communicate with nerve cells directly; rather, they release endocannabinoids, which then bind to CB1 receptors found in nearby neurons. These neurons in turn communicate directly with other nerve cells. So, the brain's immune response is regulated in an indirect manner rather than a direct one. Now, what happens with age is that your natural production of endocannabinoids decreases, which then leads to impaired immune response regulation and chronic inflammation. As noted by coauthor Dr. Andras Bilkei-Gorzo:10
Earlier research11 by this same team found that THC can help restore cognitive function in older brains, and the current study also hints at THC-containing cannabis may have valuable neuroprotective benefits in older people by quelling brain inflammation and preventing loss of brain cells. As the study was done on mice, further research is needed to confirm that the same mechanisms apply to humans, but it's compelling nonetheless. Are You Living an Inflammatory Lifestyle?Your diet can either promote or decrease inflammation. For example, foods that increase the inflammatory response in your body include:
Meanwhile, marine-based omega-3 fats have powerful anti-inflammatory effects, and are crucial for healthy brain function in general. Antioxidant-rich fruits and vegetables are also important for controlling inflammation, as is optimizing your vitamin D to a level of 60 to 80 ng/mL, ideally through sensible sun exposure. In addition to anti-inflammatory and immune-boosting properties, vitamin D receptors appear in a wide variety of brain tissue, and researchers believe optimal vitamin D levels may enhance important chemicals in your brain and protect brain cells by increasing the effectiveness of glial cells that help nurse damaged neurons back to health. A number of ubiquitous chemicals have also been implicated in inflammation, so if you struggle with fibromyalgia you'd be wise to take a close look at your choice of foods, household and personal care products. As mentioned earlier, getting enough high-quality sleep is another key treatment component for fibromyalgia. Ketogenic Diet Massively Decreases Brain InflammationResearch12 published last year suggests ketogenic diets — which are high in healthy fats and low in net carbs — are a particularly powerful ally for suppressing brain inflammation, as ketones are powerful HDAC (histone deacetylase inhibitors) that suppress the primary NF-κB inflammatory pathway. As explained by Medical Xpress,13 the defining moment of the study14 came when the team "identified a pivotal protein that links the diet to inflammatory genes, which, if blocked, could mirror the anti-inflammatory effects of ketogenic diets." A ketogenic diet changes the way your body uses energy, converting your body from burning carbohydrates for energy to burning fat as your primary source of fuel. When your body is able to burn fat, your liver creates ketones, which burn more efficiently than carbs, thus creating far less reactive oxygen species and secondary free radicals that can damage your cellular and mitochondrial cell membranes, proteins and DNA. Animals (rats) used in this study were found to have reduced inflammation when the researchers used a molecule called 2-deoxyglucose (2DG) to block glucose metabolism and induce a ketogenic state, similar to what would occur if you followed a ketogenic diet. By doing this, inflammation was brought down to levels near those found in controls. Suppressing Inflammation Improves PainSenior study author Dr. Raymond Swanson, a professor of neurology at UCSF and chief of the neurology service at the San Francisco Veterans Affairs Medical Center, commented on the results, saying:
The study also pointed out that a ketogenic diet may relieve pain via several mechanisms, similar to the ways it's known to help epilepsy.
Cyclical Ketosis for Optimal HealthEating a ketogenic diet doesn't have to be complicated or painful. My book "Fat for Fuel" presents a complete Mitochondrial Metabolic Therapy (MMT) program, complemented by an online course created in collaboration with nutritionist Miriam Kalamian, who specializes in nutritional ketosis. The course, which consists of seven comprehensive lessons, teaches you the keys to fighting chronic disease and optimizing your health and longevity. In summary, the MMT diet is a cyclical ketogenic diet, high in healthy fats and fiber, low in net carbs with a moderate amount of protein. The cyclical component is important, as long-term continuous ketosis has drawbacks that may actually undermine your health and longevity. One of the primary reasons to cycle in and out of ketosis is because the "metabolic magic" in the mitochondria actually occurs during the refeeding phase, not during the starvation phase. Ideally, once you have established ketosis you cycle healthy carbs back in to about 100 to 150 grams on days when you do strength training. MMT has a number of really important health benefits, and may just be the U-turn you've been searching for if you're struggling with a chronic health condition. You can learn more by following the hyperlinks provided in the text above. Address Emotional ContributorsSince fibromyalgia is a chronic condition, it becomes emotionally challenging in addition to the physical challenges it imposes on your life. Having a game plan to deal with your emotional well-being is especially important if you suffer from any chronic disease. If you have fibromyalgia, you might be able to trace it back to a triggering event, or you might not. Any traumatic experience has the potential to linger in your mind for a lifetime. You can have the perfect diet, the perfect exercise routine, and an ideal life; but if you have lingering unresolved emotional issues, you can still become very sick. A tool that can help release this emotional sludge is the Emotional Freedom Techniques (EFT). If you are a regular reader of my newsletter, this won't be an unfamiliar term to you. EFT is a form of bioenergetic normalization. If you have fibromyalgia, this is something that is going to be extremely helpful. You can do this yourself, at home, and it takes just a few minutes to learn. For a demonstration, see the video above. from http://articles.mercola.com/sites/articles/archive/2018/10/18/fibromyalgia-brain-inflammation-link.aspx
0 Comments
Recent data suggests that central sensitization, in which neurons in your spinal cord become sensitized by inflammation or cell damage, may be involved in the way fibromyalgia sufferers process pain. Certain chemicals in the foods you eat may trigger the release of neurotransmitters that heighten this sensitivity. Although there have been only a handful of studies on diet and fibromyalgia, the following eating rules can’t hurt, and may help, when dealing with chronic pain. Limit Sugar as Much as Possible. Increased insulin levels will typically dramatically worsen pain. So you will want to limit all sugars and this would typically include fresh fruit juices. Whole fresh fruit is the preferred method for consuming fruit products. If you are overweight, have high blood pressure, high cholesterol or diabetes, you will also want to limit grains as much as possible as they are metabolized very similarly to sugars. This would also include organic unprocessed grains. Wheat and gluten grains are the top ones to avoid. Eat fresh foods. Eating a diet of fresh foods, devoid of preservatives and additives, may ease symptoms triggered by coexisting conditions such as irritable bowel syndrome (IBS). It’s also a good idea to buy organic food when possible, as it’s best to avoid pesticides and chemicals. However, fresh is best. So if you have to choose between local, fresh, non-organic and organic but wilting – go with fresh, and clean properly. Avoid caffeine. Fibromyalgia is believed to be linked to an imbalance of brain chemicals that control mood, and it is often linked with inadequate sleep and fatigue. The temptation is to artificially and temporarily eliminate feelings of fatigue with stimulants like caffeine, but this approach does more harm than good in the long run. Though caffeine provides an initial boost of energy, it is no substitute for sleep, and is likely to keep you awake. Try avoiding nightshade vegetables. Nightshade vegetables like tomatoes, potatoes, and eggplant may trigger arthritis and pain conditions in some people. Be Careful with Your Fats. Animal based omega-3 fats like DHA and EPA have been touted as a heart-healthy food, and they may help with pain, as well. They can help reduce inflammation and improve brain function. At the same time, you want to eliminate all trans fat and fried foods, as these will promote inflammation. Use yeast sparingly. Consuming yeast may also contribute to the growth of yeast fungus, which can contribute to pain. Avoid pasteurized dairy. Many fibromyalgia sufferers have trouble digesting milk and dairy products. However, many find that raw dairy products, especially from grass fed organic sources, are well tolerated. Cut down on carbs. About 90 percent of fibromyalgia patients have low adrenal functioning, which affects metabolism of carbohydrates and may lead to hypoglycemia. Avoid aspartame. The artificial sweetener found in some diet sodas and many sugar-free sweets is part of a chemical group called excitotoxins, which activate neurons that can increase your sensitivity to pain. Avoid additives. Food additives such as monosodium glutamate (MSG) often cause trouble for pain patients. MSG is an excitatory neurotransmitter that may stimulate pain receptors; glutamate levels in spinal fluid have been shown to correlate with pain levels in fibromyalgia patients. Stay away from junk food. Limit or eliminate fast food, candy, and vending-machine products. In addition to contributing to weight gain and the development of unhealthy eating habits, these diet-wreckers may also irritate your muscles, disrupt your sleep, and compromise your immune system. from http://articles.mercola.com/sites/articles/archive/2010/01/19/foods-that-chronic-pain-sufferers-need-to-avoid.aspx
How and what you eat has radically changed over the past few decades with the all-consuming rise of the supermarket. But what price are you paying for this homogenized, cheap and convenient food? This video investigates how supermarkets have affected the food on your plate, and reveals the telltale signs that the food you buy may not have been grown in the way you think.
from http://articles.mercola.com/sites/articles/archive/2008/12/25/how-to-avoid-being-fooled-at-the-supermarket.aspx  Researchers have detected abnormalities in the brains of people with fibromyalgia, a chronic condition whose symptoms include muscle pain and fatigue. Researchers have detected abnormalities in the brains of people with fibromyalgia, a chronic condition whose symptoms include muscle pain and fatigue.Some researchers have suggested that the pain of fibromyalgia is the result of depression, but the new study suggests otherwise. The abnormalities were independent of anxiety and depression levels. Researchers evaluated 20 women diagnosed with fibromyalgia and 10 healthy women without the condition who served as a control group. The researchers performed brain imaging called single photon emission computed tomography, or SPECT. The imaging showed that women with the syndrome had "brain perfusion" -- blood flow abnormalities in their brains. The abnormalities were directly correlated with the severity of disease symptoms. An increase in blood flow was found in the brain region known to discriminate pain intensity. from http://articles.mercola.com/sites/articles/archive/2008/11/22/proof-that-fibromyalgia-is-real.aspx
People with EHS experience a variety of symptoms including headache, fatigue, nausea, burning and itchy skin, and muscle aches. These symptoms are subjective and vary between individuals, which makes the condition difficult to study, and has left experts divided about the validity of such claims. More than 30 studies have been conducted to determine what link the condition has to exposure to electromagnetic fields from sources such as radar dishes, mobile phone signals and, Wi-Fi hotspots. from http://articles.mercola.com/sites/articles/archive/2008/06/21/are-you-allergic-to-wireless-internet.aspx Dr. Jeremy Henrichs, a member of the Mahomet-Seymour school board and a physician for the University of Illinois Athletic Department, was targeted by state investigators who said they had opened an official investigation due to his opposition to mandatory masks in classrooms.1 The chilling governmental overreach is just the latest example of state and federal governments attempting to intimidate and silence those who question mask mandates and other official COVID-19 responses. Henrichs had previously voted in favor of a plan that would make mask usage optional unless infection rates rose quickly — at which point mandatory masks would be reimposed. However, due to updated CDC guidelines recommending masks for all students, the state enacted a statewide school mask mandate requiring masks for all students in class. Henrichs’ support of optional masking led to a complaint being filed, at which point the Illinois Department of Financial and Professional Regulation (IDFPR) opened an investigation to do their “due diligence.”2 State Uses Coercion and Intimidation TacticsAugust 11, 2021, Henrichs received an email from a medical investigator asking for a “detailed statement on your opinion about masks, and whether you support and will enforce a mask mandate based on your elected position as a school board member.”3 “This would fall under the unprofessional-conduct part of the Medical Practice Act,” the email added.4 It’s unclear at what point during the pandemic having an opinion contrary to the “official” rhetoric became reason for investigation, but we’re well past that point now. An attorney for Henrichs responded, questioning whether the investigation had legal standing and suggesting it was an attempt to “coerce or intimidate a public official in the performance of his public duties.” State law prohibits the intimidation of public officials going about their official duties, but IDFPR investigators said they are required to investigate every complaint about a medical professional. Why Henrichs’ opinions on masks are open for investigation is another issue entirely. In an email, a state investigator stated, “What the medical disciplinary board wants to know is if the doctor will support and enforce the mask mandate by the governor.” An IDFPR spokesperson also stated in an email, as reported by WCIA news:5
Targeted for Questioning Mandatory MaskingThe IDFPR investigation has since been called a “frightening abuse of power” by Sen. Chapin Rose, R-Mahomet, who filed a complaint in response and asked the Office of the Executive Inspector General to investigate the case.6 In a statement, Henrichs called the overreach a direct threat:7
Other regulatory bodies have issued similar threats and warnings attempting to silence physicians. The College of Physicians and Surgeons of Ontario (CPSO), which regulates the practice of medicine in Ontario, is among them. In April 2021, it issued a statement prohibiting physicians from making comments or providing advice that goes against the official narrative. According to CPSO, physicians, in isolated incidents, have been spreading blatant “misinformation” via social media, which is undermining “public health measures meant to protect all of us.” In response, they released their “Statement on Public Health Misinformation” on April 30, 2021, which reads:8
While threatening physicians with investigation and disciplinary action should they speak out regarding the many inconsistencies and questions surrounding pandemic lockdowns, masks and COVID-19 vaccines, CPSO had the gall to add that it’s not intending to stifle healthy public debate about how to “best address aspects of the pandemic.” “Rather, our focus is on addressing those arguments that reject scientific evidence and seek to rouse emotions over reason,” it added.9 IDFPR Issues Apology to HenrichsAfter backlash, including Rose’s call for an investigation into IDFPR’s actions, the agency issued a letter of apology to Henrichs, backpedaling on their inquiry. In an email to Henrichs’ attorney, Dina Torrisi Martin, general counsel for IDFPR, stated:10
Mario Treto Jr., IDFPR’s secretary, also stated that a preliminary review of the complaint has concluded with the strong recommendation that the complaint be closed. In a statement, Henrichs said he appreciated the apology, but “until this complaint has, in fact, formally been dismissed,” he has “nothing further to say at this time.”11 State Boards Threaten Licenses, Don’t Define ‘Misinformation’A spokeswoman for Illinois Gov. JB Pritzker, Jordan Abudayyeh, stated, “The Pritzker administration has not and will not seek disciplinary action against the professional licenses of individuals who disagree with the mask mandate.”12 Yet, according to a statement released by the Federation of State Medical Boards (FSMB), they absolutely could. In a news release titled, “Spreading COVID-19 Misinformation May Put Medical License at Risk,” FSMB stated that the “dramatic increase in the dissemination of COVID-19 vaccine 'misinformation' and 'disinformation' by physicians and other health care professionals on social media platforms, online and in the media” led to the release of their latest threat, which they called a “statement”:13,14
Markedly absent from the statement is a definition of what constitutes “misinformation,” leaving the word wide open for interpretation. It’s not only physicians that are being hunted down but also academics. Virtually anyone who speaks out about data that go against the official COVID propaganda can be labeled a dangerous “agent of misinformation,” which is what happened to Harvard epidemiologist Martin Kulldorff, who wrote a paper against lockdowns but couldn’t get it published. Kulldorff and colleagues soon banded together to write the Great Barrington Declaration,15 which calls for “focused protection” of the elderly and those in nursing homes and hospitals, while allowing businesses and schools to remain open. Soon after, they too were attacked and accused of spreading misinformation and being “COVID deniers.”16 Professor Mark Crispin Miller, who has taught classes on mass persuasion and propaganda at the New York University Steinhardt School of Culture, Education and Human Development for the last two decades, is another example. After challenging students to investigate current propaganda narratives surrounding mask mandates, Miller was placed under conduct review for spreading “dangerous misinformation.” Miller fought back, suing 19 of his department colleagues for libel after they signed a letter to the school dean demanding a review of Miller’s conduct.17 Miller also launched a petition to New York University in support of academic freedom, free speech and free inquiry, without which he states, “‘education’ … will be mere training for compliance, stunting students’ minds instead of opening them — a practice fatal to democracy, and, finally, to humanity itself.”18 Are State Boards Maintaining Hit Lists?Jumping on the libel bandwagon, MedPage Today conducted an investigation into 20 physicians it says are spreading “COVID-19 misinformation,” including me, noting that “not one of 20 physicians who've peddled such falsehoods has been disciplined by their state licensing agency for doing so.”19 MedPage Today contacted 10 states that license physicians, apparently to ask them why they haven’t disciplined physicians for spreading undefined “misinformation.” In Illinois, IDFPR stated that if the agency "determines a licensee committed violations against the Act that regulates their profession, an appropriate course of action will be taken. Complaints filed with and investigations undertaken by IDFPR are confidential, unless and until a public complaint or discipline is issued by the Department."20 From MedPage Today’s investigation, it seems that states have put together lists of the people they’re targeting to delicense, but none has taken action against the physicians they’re accusing of spreading unidentified “bad info.” Perhaps that’s because sharing information isn’t a crime, but stifling it — and engaging in unfounded threats and intimidation — is. from http://articles.mercola.com/sites/articles/archive/2021/08/30/doctors-targeted-for-questioning-mandatory-masking.aspx The oft-repeated refrain right now is that we're in a "pandemic of the unvaccinated," meaning those who have not received the COVID jab make up the bulk of those hospitalized and dying from the Delta variant. For example, August 20, 2021, England's chief medical officer professor Chris Whitty tweeted:1,2
Curiously, if you take the time to actually look at the data, you'll find that this blanket statement is rather deceptive. Here's a graphic published in the Evening Standard, sourced from Public Health England:3 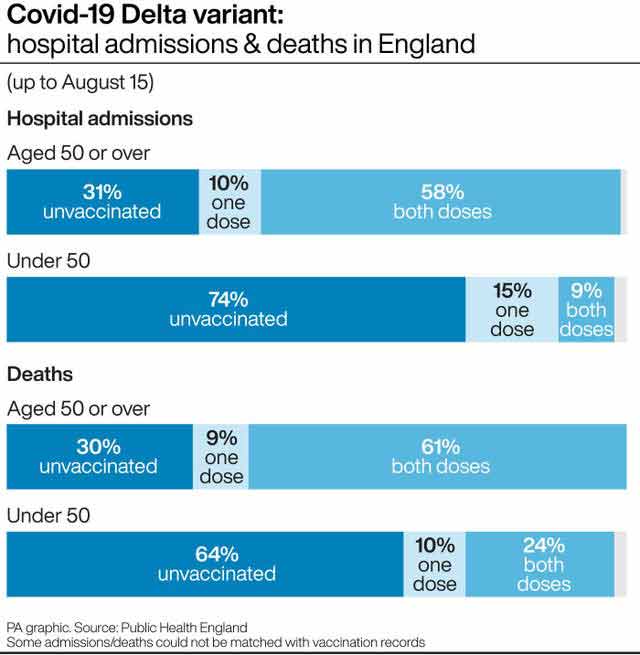
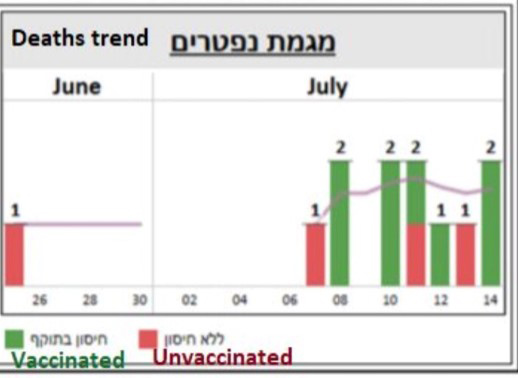
As you can see, as of August 15, 2021, 58% of COVID patients admitted to hospital who were over the age of 50 had actually received two doses of COVID injections and 10% had received one dose. So, partially or fully "vaccinated" individuals made up 68% of hospitalizations. Only in the 50 and younger category were a majority, 74%, of hospitalizations among the unvaccinated. Whitty, however, completely neglected to differentiate between the age groups. The same applies to deaths. Unvaccinated only make up the majority of COVID deaths in the under-50 age group. In the over-50 group, the clear majority, 70%, are either partially or fully "vaccinated." It's also unclear whether hospitals in the U.K. (and elsewhere) are still designating anyone who is admitted and tests positive with a PCR test as a "COVID patient." If so, people with broken bones or any number of other health problems who have no symptoms of COVID-19 at all might be unfairly lumped into the "unvaccinated COVID patient" total. Israeli Data Show COVID Jab Is Failing in Over-50sIn Israel, where vaccine uptake has been very high due to restrictions on freedom for those who don't comply,4 data show those who have received the COVID jab are 6.72 times more likely to get infected than people with natural immunity.5,6,7 The fully "vaccinated" also made up the bulk of serious cases and COVID-related deaths in July 2021, as illustrated in the graphs below.8 The red is unvaccinated, yellow refers to partially "vaccinated" and green fully "vaccinated" with two doses. By mid-August, 59% of serious cases were among those who had received two COVID injections,9 mirroring the data coming out of the U.K. 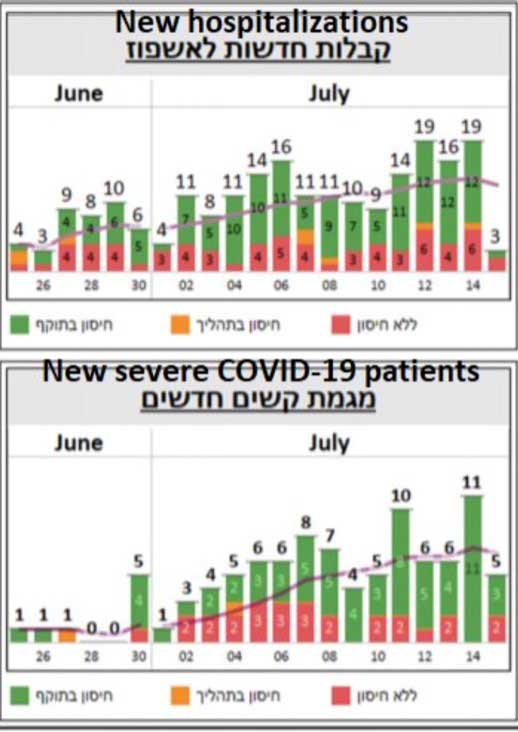
In an August 16, 2021, Science article,10 Israeli Minister of Health Nitzan Horowitz is quoted saying the nation has entered a "critical time" in the race against the pandemic. Horowitz allegedly was given a third booster shot August 13, 2021, the day they began offering a third dose to people over the age of 50. From Public Health England's data, it seems clear that the COVID shots are failing to protect people over the age of 50 in the U.K. as well, so it's probably only a matter of time before booster shots are rolled out there too. And, provided the COVID injections are the same irrespective of country, there's every reason to assume the same trends will emerge in other countries, including the U.S. This is precisely what Ran Balicer, chief innovation officer at Clalit Health Services, Israel's largest health maintenance organization (HMO), told Science: "If it can happen here, it can probably happen everywhere."11 Israeli Data Considered the Best AroundThe data coming out of Israel is considered by many to be the best we have, and can give us a glimpse of what to expect elsewhere. As explained by Science magazine:12
Where Will It End?According to Science magazine, breakthrough cases are now multiplying at breakneck speed. "There are so many breakthrough infections that they dominate and most of the hospitalized patients are actually vaccinated," Uri Shalit, a bioinformatician at the Israel Institute of Technology told Science.14 Nearly 1 million Israelis over the age of 50 have now received a third booster of Pfizer's mRNA shot. Time will tell whether this will worsen the rate of breakthrough cases or tame it. Dvir Aran, a biomedical data scientist at the Israel Institute of Technology doesn't seem very hopeful, telling Science the surge is already so steep, "even if you get two-thirds of those 60-plus [boosted], it's just gonna give us another week, maybe two weeks until our hospitals are flooded" again.15 The obvious question is, what then?! Will the answer be a fourth injection before the year is over? Will we be looking at quarterly injections? Monthly injections? Biweekly? Weekly? Where and when does it end? It is fairly easy to predict that this can only end very badly. US Tracks Only Fraction of Breakthrough InfectionsUnfortunately, we cannot rely on U.S. data to get a clear idea of how the COVID shots are working, as the U.S. Centers for Disease Control and Prevention has chosen not to track all breakthrough cases. As reported by ProPublica,16 May 1, 2021, the CDC stopped tracking and reporting all breakthrough cases, opting to log only those that result in hospitalization and/or death. As noted in the article, this irrational decision has "left the nation with a muddled understanding of COVID-19's impact on the vaccinated." It also prevents us from understanding how variants are spreading and whether those who have received the jab can still develop so-called "long-haul syndrome." Individual states are also setting their own criteria for how they collect data on breakthrough cases, and this patchwork muddies the waters even further. Despite these limitations, what little data we do have is starting to mirror that of Israel and the U.K. August 18, 2021, the CDC released three reports,17,18,19 which show the protection you get from the COVID shot is rapidly waning.
Vaxxed Are Up to 13 Times More Likely to Get Delta VariantWhile the U.S. is lax about recording breakthrough infections, researchers in Israel have some breaking news: They have been keeping track, and their studies22 show that vaccinated individuals are up to 13 times more likely to get the Delta variant of COVID-19 than those who were not vaccinated, but had recovered from a COVID infection. As explained by ScienceMag:23 The study "found in two analyses that people who were vaccinated in January and February were, in June, July and the first half of August, six to 13 times more likely to get infected than unvaccinated people who were previously infected with the coronavirus. In one analysis, comparing more than 32,000 people in the health system, the risk of developing symptomatic COVID-19 was 27 times higher among the vaccinated, and the risk of hospitalization eight times higher." The study also said that, while vaccinated persons who also had natural infection did appear to have additional protection against the Delta variant, the vaccinated were still at a greater risk for COVID-19-related-hospitalizations compared to those without the vaccine, but who were previously infected. Vaccinees who hadn't had a natural infection also had a 5.96-fold increased risk for breakthrough infection and a 7.13-fold increased risk for symptomatic disease. One thing to note here is that the wording of this is important: The study does not say that getting a vaccine helps protect you if you've had a natural infection; rather, it says that natural protection helps boost the vaccine. Either way, even if you do have natural infection in combination with the vaccination, vaccinees are still at an increased risk for a breakthrough infection. "This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity," the study authors concluded. Fully Vaxxed Speak OutBack America, in an August 24, 2021, article,24 The Defender cites data from seven states (California, Colorado, Massachusetts, Oregon, Utah, Vermont and Virginia) that keep more detailed records than most. In six of these states, breakthrough infections accounted for 18% to 28% of all new COVID diagnoses in the past several weeks, as well as 12% to 24% of all COVID-related hospitalizations. In Los Angeles, breakthrough cases have risen from 5% in April and 13% in July to a current of 30%. Fully vaxxed celebrities and elected officials have now started speaking out after getting COVID. As reported by The Defender: 25
CDC Has Also Hidden Breakthrough Cases in Other WaysThe CDC also cooked the books on COVID breakthrough cases in other ways. Originally, the CDC recommended labs use a CT of 4026 when testing for SARS-CoV-2 infection. This, despite using a CT above 35 was known to create a false positive rate of 97%.27 By using an exaggerated CT, healthy people were deemed stricken with COVID-19. In May 2021, the CDC lowered the CT from 40 to 28 or lower — but only when doing PCR testing on individuals who have received the COVID jab.28 Unvaccinated were still tested using a CT of 40. The end result is obvious: "Vaccinated" individuals became far less likely to test positive for SARS-CoV-2 infection while unvaccinated were still exceedingly getting false positives. As noted by Off-Guardian:29
How the CDC Invented the 'Pandemic of Unvaxxed' NarrativeThe CDC also played fast and loose with the data when it invented the "pandemic of the unvaccinated" narrative30 that we're now being indoctrinated with. In a July 16, 2021, White House press briefing,31 CDC director Dr. Rochelle Walensky claimed "over 97% of people who are entering the hospital right now are unvaccinated." As it turns out, that statistic is based on hospitalization data from January through June 2021, when the majority of Americans had not yet gotten the COVID jab. January 1, 2021, only 0.5% of the U.S. population had received a COVID shot. By mid-April, an estimated 31% had received one or more shots,32 and as of June 30, just 46.9% were "fully vaccinated."33 COVID Shots 'Proven to Cause More Harm Than Good'While the official narrative is that the COVID shots may be "less than perfect" but are still better than the alternative (i.e., getting the infection when you're unvaccinated), Dr. Bart Classen published a study34 in the August 2021 issue of Trends in Internal Medicine, disputing this claim. The study,35 "U.S. COVID-19 Vaccines Proven to Cause More Harm than Good Based on Pivotal Clinical Trial Data Analyzed Using the Proper Scientific Endpoint, 'All Cause Severe Morbidity,'" details a core problem with Pfizer's, Moderna's and Janssen's (Johnson & Johnson) trials. All three employ a surrogate primary endpoint for health, namely "severe infections with COVID-19." This, Classen says, "has been proven dangerously misleading," and many fields of medicine have stopped using disease-specific endpoints in clinical trials and have adopted "all-cause mortality and morbidity" instead. The reason for this is because if a person dies from the treatment or is severely injured by it, even if the treatment helped block the progression of the disease they're being treated for, the end result is still a negative one. To offer an extreme example of what you can do with a disease-specific endpoint, you could make the claim that shooting people in the head is a cure for cancer, because no one who got the treatment — who got shot in the head — died from cancer. When reanalyzing the clinical trial data from these COVID shots using "all-cause severe morbidity" as the primary endpoint, the data reveal they actually cause far more harm than good. The proper endpoint was calculated by adding together all severe events reported in the trials, not just COVID-19 but also all other serious adverse events. By doing this, severe COVID-19 infection gets the same weight as other adverse events of equivalent severity. According to Classen:36
To make the above numbers more clear and obvious, here are the prevention stats in percentages:
Where Do We Go From Here?If you've already gotten one or two shots, there's nothing you can do about that. It seems pretty obvious, though, if you objectively analyze the data, that your best bet is to say no to any and all future boosters, as each additional shot can magnify the damage and increase your risk of serious side effects. If you develop symptoms of SARS-CoV-2 infection, there are several treatment protocols available that have been shown to be effective. Options include the Zelenko protocol,37 the MATH+ protocols38 and nebulized hydrogen peroxide, as detailed in Dr. David Brownstein's case paper39 and Dr. Thomas Levy's free e-book, "Rapid Virus Recovery." Whichever treatment protocol you use, make sure you begin treatment as soon as possible, ideally at first onset of symptoms. Also, realize that if you've gotten one or more COVID shots, your risk of severe infection may actually be greater, not lesser, than had you not gotten the injections. This appears particularly true if you're over the age of 50. So, do not delay treatment if you develop symptoms. from http://articles.mercola.com/sites/articles/archive/2021/08/30/fully-vaccinated-covid-deaths.aspx In this interview, Thomas Lewis, Ph.D., and Dr. Michael Carter explain how biomarker panels can help you take control of your health by identifying underlying chronic infections that might be sabotaging your health. Lewis is a microbiologist with a Ph.D. from MIT and certifications from the Harvard School of Public Health and Carter is an integrative physician. They run a company that performs diagnostic testing to guide patients through a process of diagnosing various ailments. Biomarkers such as D-dimer, fibrinogen, clotting factors and auto antibodies, which are largely ignored by the mainstream, can clue you in on where you lie on a health/disease continuum. Importantly, poor COVID outcomes are rare unless you have two or more comorbidities, and in the last year, they’ve developed a more refined way of assessing an individual’s COVID-19 risk using a panel of specific markers associated with inflammation and blood clotting. Their testing helps YOU understand where you are on the health-disease continuum. In their model, you are not either sick or well — you are somewhere on this continuum. Find out where you are and then work to improve your status. “Really, it's your chronic health status that helps you figure out where you are in the continuum for COVID risk,” Lewis explains. The same goes for the COVID shot. According to Lewis, whether you got COVID-19 or the vaccine, the risk factors that determine whether you’ll have a serious bout of COVID-19 or experience more serious adverse events from the shot are identical. The Role of Underlying InfectionsUnderlying or latent infections can play a significant role not only in chronic disease but also in SARS-CoV-2 infection. Judy Mikovits, Ph.D., has pointed out the role of retroviruses and coinfections with pathogens such as borellia and babesia in leading to less favorable outcomes in COVID. Her hypothesis is that SARS-CoV-2 in and of itself is not the primary cause of COVID-19. She’s convinced there must be a coinfection along with SARS-CoV-2 that suppresses or compromises your immune system in order for symptomatic COVID-19 to occur. Carter and Lewis have discovered a number of infectious pathogens that are even more prolific than those highlighted by Mikovits, and which appear central in triggering many chronic conditions that then predispose you to more severe COVID-19. Primary among those are bacteria involved in periodontal disease (periodontitis). You don’t have to have oral issues or root canals to have a high burden of periodontal pathogens. The Lewis/Carter team test for these pathogens using an oral DNA home test kit. Another is chlamydia pneumoniae, a respiratory pathogen that 60% to 70% of older adults have antibodies against. Chlamydia pneumoniae plays a role in several common age-related conditions, including Alzheimer’s disease, heart disease and rheumatoid arthritis. Unfortunately, few are ever tested for the presence of this organism. According to Lewis and Carter, inflammatory markers and clotting markers such as C-reactive protein, fibrinogen, uric acid, the neutrophil-to-lymphocyte ratio, D-dimer, and sedimentation (SED) rate are strongly associated with innate immune response activity and chronic infections, which in turn correlate with COVID-19 severity.
So, to clarify the hypothesis presented by Lewis and Carter, the conventional view is that these infections, once they've generated an IgG antibody response, no longer pose a threat to your body. But this isn’t the case. They can indeed lay dormant only to later contribute to chronic diseases that, on the surface, appear to have nothing to do with a pathogenic infection. The book by Paul Ewald titled, “Plague Time: The New Germ Theory of Disease,” written in 2000, explains well this conundrum. How to Identify Underlying InfectionsThe clinical approach to identifying whether an underlying infection is at play in a particular disease is to look at antibody levels. Immunoglobulin G (IgG) is reflective of long-term protection and also happens to be the most common antibody, found in blood and other body fluids. It protects against both viral and bacterial infections and tends to be elevated when the infection has reached a chronic state. Immunoglobulin M (IgM) is associated with acute responses to infections and is found primarily in your blood and lymph. It’s the first antibody to be made when your body encounters a new pathogen. Carter explains:
In summary, if you have elevations (or suppressions) in white blood cell markers, then you likely have an infectious process going on in your body. There’s also typically a direct correlation between your antibody level and the risk of disease, so the higher your antibody level, the greater your risk of chronic disease and poor COVID / JAB outcomes. PCR testing can be useful for identifying a specific pathogen. However, if excessively high cycle thresholds (CTs) are used (as has been the rule when testing for SARS-CoV-2), the test becomes useless, as it can find even a single molecule if run at a high-enough CT. So, the CT needs to be below 26 to avoid false positives. Review of Lewis and Carter’s ResearchBefore we go further, here’s how Lewis describes their research, and how it can improve your health and medical decisions:
Treating Chronic Versus Acute InfectionsCarter and Lewis have developed a pretreatment program, followed by a variety of treatment strategies aimed at chronic infections. As you might expect, the chronic infection treatments involve more aggressive approaches, and will depend on whether the infection is caused by bacteria, viruses or parasites. The biggest factor for effective treatment is eradicating pathogens hiding in biofilm, which takes time. (We do not address the use of specific remedies in this interview, as each patient must be tested, seeing how there’s such a broad array of potential causal factors.) As noted by Lewis, even if you use a broad-spectrum anti-infective, such as ozone, you’ll rarely eradicate enough of the chronic phase of these organisms, as they shelter inside biofilms or inside your cells — including your white blood cells. that are very difficult to get into. These pathogens are often referred to as “obligate intracellular pathogens.” The “obligate” part infers that these harmful organisms rob your energy by mimicing to be your mitochondria. He explains:
The Role of Vitamin DA basic intervention that is really important for shoring up your immune system is vitamin D. Vitamin D is really a pro-hormone and hormones regulate physiological processes. I believe vitamin D optimization — making sure your blood level is between 60 ng/mL and 80 ng/mL (150 nmol/L and 200 nmol/L) — is one of the easiest, least expensive and most important things you can do to avoid infections of all kinds, including COVID-19. The activated form of “vitamin” D is produced in your liver when you have an infection and it is strongly antibiotic. Lewis and Carter recently completed a study in which they looked at the vitamin D level compared to neutrophil and lymphocyte ratio. Lewis explains:
They’ve also found a similar correlation between chronic infection and free cholesterol (not total cholesterol). This correlation appears particularly strong in those with cancer, who typically have a free cholesterol level of 50 ng/mL and above. An optimal level is thought to be somewhere between 5 ng/mL and 20 ng/mL, with the healthiest of people typically falling between 5 ng/mL and 15 ng/mL. When free cholesterol is elevated, you’re more prone to tissue destruction, as cholesterol is an important repair molecule. Since your cholesterol level can indicate your tissue repair capability, it is also included in Lewis’ and Carter’s COVID panel.
How Do You Know if an Infection Is Chronic?One way to determine whether you’re suffering from an acute or chronic infection is to look at the half-life of the factors being measured. Lewis explains:
What’s in the Panel?Speaking to the issue of what the panel Lewis and Carter developed contains, Carter explains:
In addition to helping you evaluate your chronic disease risk, this panel will also help you assess your COVID-19 risk. They also offer an advanced panel that is even more comprehensive. It costs about $400 and includes a one-hour consultation to help you understand what all the markers mean. As noted by Lewis, “It's all about where do you lie on the health/disease continuum. We very accurately are placing people on that, and there's not a marker we test for that's not modifiable through lifestyle or other appropriate interventions. We're not treating symptoms. We're going right at the disease.” Where to Get the PanelIf you’re interested in ordering this panel, go to HealthRevivalPartners.com. If you want to get the comprehensive COVID / JAB risk screening panel, go to www.healthrevivalpartners.com/post-jab-tests. You will be asked to fill out a questionnaire, after which you receive a requisition to have your blood drawn at a LabCorp. The report you get will be a comprehensive and detailed report from Health Revival Partners in addition to the standard lab report. Carter explains:
Building a Stronger Foundation for Functional MedicineAgain, to learn more, and to join the Health Revival Partners’ chronic disease support program, go to HealthRevivalPartners.com. In closing, Lewis notes:
from http://articles.mercola.com/sites/articles/archive/2021/08/29/identifying-underlying-chronic-infections.aspx By Dr. Mercola One of the simplest and most enjoyable ways to up the health ante of your meals is by adding herbs and spices, and in the realm of spices, turmeric and its active ingredient curcumin may be king. If you're a fan of curry, you're probably also a fan of turmeric, as this is the yellow-orange spice that makes the foundation of many curry dishes. It's a great addition to your diet, but to get the full benefits curcumin has to offer, look for a turmeric extract that contains 100 percent certified organic ingredients and at least 95 percent curcuminoids. Research is emerging showing that this potent spice may play a beneficial role in preventing and treating numerous chronic diseases, and may offer promise in helping people deal with obesity and obesity-related metabolic diseases. Does Curcumin Boost Weight Loss?Research in the European Journal of Nutrition suggests that curcumin may be useful for the treatment and prevention of obesity-related chronic diseases, as the interactions of curcumin with several signal transduction pathways -- the process by which biological functions are recognized -- also reverse insulin resistance, hyperglycemia, hyperlipidemia, and other inflammatory symptoms associated with obesity and metabolic disorders. Curcumin is known for its potent anti-inflammatory properties, and chronic inflammation is the hallmark of most chronic disease, including diabetes, arthritis, and heart disease. But many people are not aware that obesity contributes to a state of low-grade, chronic inflammation in your body that can trigger metabolic disorders such as insulin resistance and type 2 diabetes. Curcumin appears to modulate several cellular transduction pathways that contribute to this damaging process. As a result, researchers concluded:
Past research has revealed similar findings, including that curcumin reduces the formation of fat tissue by suppressing the blood vessels needed to form it. As the researchers stated:
Weight Loss is Just the Icing on the CakeThe benefits of curcumin go way beyond weight loss. The compound has been shown to influence more than 700 genes, and it can inhibit both the activity and the synthesis of cyclooxygenase-2 (COX2) and 5-lipooxygenase (5-LOX), as well as other enzymes that have been implicated in inflammation. But that's not all. Curcumin currently has the most evidence-based literature supporting its use against cancer than any other nutrient. Interestingly this also includes the metabolite of curcumin and its derivatives, which are also anti-cancerous. Best of all, curcumin appears to be safe in the treatment of all cancers. Researchers have found that curcumin can affect more than 100 different pathways, once it gets into the cell. More specifically, curcumin has been found to:
However, much of curcumin's power seems to lie in its ability to modulate genetic activity and expression -- both by destroying cancer cells and by promoting healthy cell function. As such, evidence suggests curcumin may play a beneficial role in the following conditions:
Tips for Using Curcumin TherapeuticallyYou can use turmeric in your cooking (choose a pure turmeric powder, rather than a curry powder, as at least one study has found that curry powders tend to contain very little curcumin), but you may also want to consider taking it in supplement form. For many this is a more convenient method to obtain the potential health benefits, especially if it is from a high-quality organic source, and also if you don't particularly enjoy the taste of curry. Unfortunately, at the present time there really are no formulations available for the use against cancer, as relatively high doses are required and curcumin is not absorbed that well. According to Dr. William LaValley, one of the leading medicine cancer physicians I personally know, typical anticancer doses are up to three grams of good bioavailable curcumin extract, three to four times daily. One work-around is to use the curcumin powder and make a microemulsion of it by combining a tablespoon of the powder and mixing it into 1-2 egg yolks and a teaspoon or two of melted coconut oil. Then use a high-speed hand blender to emulsify the powder. Another strategy that can help increase absorption is to put one tablespoon of the curcumin powder into a quart of boiling water. It must be boiling when you add the powder as it will not work as well if you put it in room temperature water and heat the water and curcumin. After boiling it for ten minutes you will have created a 12 percent solution that you can drink once it has cooled down. It will have a woody taste. The curcumin will gradually fall out of solution however. In about six hours it will be a 6 percent solution, so it's best to drink the water within four hours. Be aware that curcumin is a very potent yellow pigment and can permanently discolor surfaces if you aren't careful. Be Sure Your Weight Loss Strategy is ComprehensiveIt can't hurt to add curcumin to your comprehensive weight loss program, but it should not be your only strategy for weight loss if you're currently overweight or obese. You can read an in-depth explanation of the common factors that contribute to weight loss here, but the key is the quality of your calories and exercise. Typically you will need to replace grains and sugars, including fructose, with high-quality protein and fats AND add in high-intensity exercise training like Peak Fitness. I realize that this might conflict with your previous understanding of a healthy diet, but that is clearly what the bulk of the science and anecdotal evidence supports. For more comprehensive details, please see my nutrition plan, which is divided into beginner, intermediary and advanced, so that you can slowly work your way toward achieving your weight loss goals. from http://articles.mercola.com/sites/articles/archive/2011/09/22/could-this-spice-actually-help-weight-loss.aspx The past 18 months has provided Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases and chief medical adviser to the president of the U.S., ample opportunity to truthfully share information about an ongoing health situation. However, as his statements have been tracked, it appears he has not taken the higher path of truth that would have helped American’s make smart decisions. Instead, he has engaged in what the daily online magazine Slate labeled “noble lies.” The writer asks this question: “Do we want public health officials to report facts and uncertainties transparently? Or do we want them to shape information?”1 Although this is a question only you can answer for yourself, Fauci’s inaccurate representation of the truth likely has a deeper meaning than what philosophers define as a noble lie. It may be difficult to untangle the reason behind the lies, but there are several theories as to why Fauci believes he can determine what is true and what is not. The lab leak theory was first publicly proposed by then-President Trump2 and vehemently denied by Fauci. Experts postulate the reason the media did not further explore the idea was the announcement politically polarized it, burying the possibility it might be fully and independently investigated.3 Yet, objective accurate news reporting may only be an illusion since, as TechStartUps reports,4 six corporations control 90% of what is published in America as of September 2020. And, Vanguard and Blackrock are the top investors in each of those six corporations, namely Comcast,5 Disney,6 ViacomCBS,7 News Corp,8 and AT&T.9 As you may note, there are only five corporations listed above. That’s because TechStartUps listed Viacom and CBS separately as the merger between the companies had only recently closed.10 In other words, the five or six supposedly competitive corporations vying for 90% of the American public are really controlled by two investment firms, Vanguard and Blackrock. And, in an interesting twist of events, Vanguard is the top investor in Blackrock.11 Whether Fauci is politicizing the truth, or the news media is picking and choosing the truth they tell you to serve their own financial needs, it is highly likely that what you read in mainstream news media is exactly what serves the purposes of an elite class that controls “what we read, watch or listen to.”12 What Is a Noble Lie?The origin of a “noble lie” is from Plato’s Republic,13 a book written in 380 B.C., which essentially is a discussion of the meaning and nature of justice.14 Without getting too embroiled in the philosophical argument over truth and lies, it's important to note that Immanuel Kant (1724-1804) was a central figure in the development of modern philosophy.15 His position was that lying was never morally acceptable,16 something few contemporary philosophers agree with. Philosophically, there are two lies that are generally believed to be acceptable. The first prevents catastrophic events and the second are “white lies,” where the consequences are considered by the speaker to be insignificant.17 A noble lie falls under the category of paternalistic lies. The American Psychological Association18 states this about lies with paternalistic motives: “Many lies that are intended to help others require the deceiver to make assumptions about whether lying serves others’ best interest.” In other words, Fauci may be functioning under the delusion that he has the right and responsibility of making an assumption about whether the lies he tells are serving the best interest of those who have the full capacity and capability of understanding the science and making up their own mind. One of the Lies Began With MaskingAlthough Fauci’s string of lies about the public health response and origins of COVID-19 are far-reaching, some of the first he told were about the effectiveness of wearing masks to reduce the spread of the virus. In the short video below, Rep. Jim Jordan, D-Ohio, gives a scathing account of Fauci’s vacillating recommendations regarding masking in public. Fauci was appointed the director of the NIAID in 1984, which you would think would make him an expert by 2020 on infectious disease transmission. However, he hasn’t been able to make up his mind during the entire pandemic what his “expert” advise is on mask wearing. Fauci explained his first recommendation not to wear masks during a March 2020 “60 Minutes” interview, saying using a mask in the community was unnecessary, and specifically:19
In other words, based on his expert knowledge, wearing a mask in the community would not be effective. But just three months later in an interview on TheStreet, Fauci justified changing his expert advice as he talked about some of the characteristics of the illness:20
The only thing is, as the director of NIAID who focuses on infectious diseases, Fauci has to have been aware of studies demonstrating the asymptomatic nature of other respiratory viral illnesses such as influenza21 and statements on the CDC website that flu “can cause mild to severe illness, and at times can lead to death.”22 In other words, while we know that a SARS-CoV-2 infection can trigger symptoms like flu, it seems odd that Fauci’s characterization of COVID-19 spread is something “I've quite frankly never seen anything like.” Fauci Claims We Can Crush COVID as Vaccinated People Get SickDuring the same interview he said the reason he recommended not wearing masks in the beginning was to avoid mass panic that might lead to a shortage of masks for health care workers.23 Fauci’s unique brand of justifying behavior, like his flip-flopping over mask wearing, has also slipped into his reasoning for the shot program. In an interview with MSNBC, he says:24
From here he advises that all people who have been vaccinated to wear a mask indoors to prevent the spread of the infection. His explanation is that the delta variant has "changed the entire landscape." However, as we know from other viruses, the coronavirus will continue to mutate and change, which means, from Fauci's explanation, people will always be wearing masks to prevent the spread of a continually mutating virus. The interviewer points out that as the virus continues to change, it means we won't be able to "turn the page on coronavirus, because there might be new variants ..."25 to which Fauci responds, "It doesn't have to be if the overwhelming majority of the people in this country get vaccinated. We could nail this down by just crushing it."26 So, within the space of four minutes Fauci said that without a doubt, people can get infected after vaccination and carry enough virus to transmit the infection — BUT — if the overwhelming majority of people are vaccinated the virus would be crushed. Fact Checkers Believe What’s Missing Is ContextThe evidence about mask effectiveness does not change based on one virus among well over 200 different types27 that affect the respiratory system. February 5, 2020, Fauci wrote in an email: “The typical mask you buy in the drug store is not really effective in keeping out virus, which is small enough to pass through the material.”28 June 2, 2021, under the Freedom of Information Act (FOIA), BuzzFeed received 3,234 pages of Fauci’s emails.29 Some of these emails concerned the changing mask recommendations for the community. The writer of a fact-checking article in USA Today wrote that guidance on masks and other mitigating measures were updated as scientists learned more about the virus. Ultimately, the writer defends the information released through the FOIA, claiming that the emails are missing context.30 In other words the supposedly most superior infectious disease expert in the U.S. only developed a greater understanding about the effectiveness of masks against viruses, which have been used and studied for decades,31 as the SARS-CoV-2 infection evolved over 2020. Half-Truths About Gain-of-Function Research and Herd ImmunityGain-of-function research can make a pathogen more infectious or more lethal. The moratorium on gain-of-function research that began in October 2014 was lifted in 2017 so federal money could once again be used for this purpose.32 In this short video, Jordan quickly illustrates the change in Fauci’s position over the past 18 months, saying:33
Jordan goes on to say, “Talk about being all over the board. I’ll tell you what’s negligent. Negligent is Dr. Fauci’s ever-changing statements to the American people regarding the subject matter that this committee should be looking into.” In June 2021, The Nation pointed out that as he testified before the U.S. Senate in May, “Fauci was asked by Rand Paul, ‘Do you still support [National Institutes of Health] funding of the lab in Wuhan?’” to which Fauci replied “with all due respect, you are entirely and completely incorrect.”34 However, this half-truth, told after his admission that it would have been negligent not to fund the lab in China, is not a noble lie as it doesn't protect anyone except Fauci. Later in his testimony, Fauci hedged: “Dr. Baric is not doing gain-of-function research, and if it is, it is according to the guidelines, and it is being conducted in North Carolina.”35 So, does this mean research is being done, or it isn't? Fauci’s lies include his definition of herd immunity. A New York Times36 article in December 2020 discussed Fauci’s perspective on herd immunity. The reporter noted that in the early months of 2020, Fauci cited a 60% to 70% estimate. Later in the year he boosted this to 70% to 75% during television interviews. In an interview with CNBC news December 16, 2020, he said, “I would think that you would need somewhere between 70, 75, maybe 80%.”37 In a telephone interview with The New York Times the very next day, Fauci admitted that he had slowly been moving the goal posts, “partly based on new science and partly based on his gut feeling that the country is finally ready to hear what he really thinks.”38 Fauci claimed he had delayed raising the estimate because of vaccine hesitancy, saying, “We really don’t know what the real number is. I think the real range is somewhere between 70 to 90 percent. But, I’m not going to say 90 percent.”39 Can Fauci Predict the Future?What is Fauci saying? In his own words, he was raising the estimate for the target range for herd immunity to promote more people taking the vaccine. However, infectious disease specialists are not necessarily social behavioral experts and cannot predict how people will react to information. Fauci claims he downplayed the importance of wearing masks to avoid a shortage for health care professionals. However, does this mean he knew masks were not effective against viral transmission and were less likely to be effective in the community, or that he just didn't care? The question remains, do you want a public health official who reports the facts transparently, or one who manipulates your behavior to take specific actions? from http://articles.mercola.com/sites/articles/archive/2021/08/28/when-noble-lies-become-blatant-lies.aspx |
Nia Pure NatureThe Provider of premium Quality Health Products To Live Better Lives Archives
March 2022
Categories |
 Chronic pain is a pervasive issue and fibromyalgia is a very common form. It is a chronic condition whose symptoms include muscle and tissue pain, fatigue, depression, and sleep disturbances.
Chronic pain is a pervasive issue and fibromyalgia is a very common form. It is a chronic condition whose symptoms include muscle and tissue pain, fatigue, depression, and sleep disturbances. Electromagnetic Hypersensitivity Syndrome (EHS) is a condition in which people are highly sensitive to electromagnetic fields. In an area such as a wireless hotspot, they experience pain or other symptoms.
Electromagnetic Hypersensitivity Syndrome (EHS) is a condition in which people are highly sensitive to electromagnetic fields. In an area such as a wireless hotspot, they experience pain or other symptoms. RSS Feed
RSS Feed
