|
Mass psychosis is defined as “an epidemic of madness” that occurs when a “large portion of society loses touch with reality and descends into delusions.” The witch trials of the 16th and 17th centuries are a classic example. We’re now in the middle of another mass psychosis, induced by relentless fearmongering coupled with data suppression and intimidation tactics of all kinds. The 20-minute video above, “Mass Psychosis — How an Entire Population Becomes Mentally Ill,” created by After Skool and Academy of Ideas,1 explains the tactics used to seed and nurture mental illness on a grand scale. Fearmongering Breeds InsanityA number of mental health experts have expressed concern over the blatant panic mongering during the COVID-19 pandemic, warning it can have serious psychiatric effects. For example, in a December 22, 2020, article2 in Evie Magazine, S.G. Cheah discussed the emergence of mass insanity caused by “delusional fear of COVID-19.”
In a December 2020 interview (below), psychiatrist and medical legal expert Dr. Mark McDonald4 also went on record stating “the true public health crisis lies in the widespread fear which morphed and evolved into a form of mass delusional psychosis.” He went so far as to refer to the outside of his home or office as the “outdoor insane asylum,” where he must assume “that any person that I run into is insane” unless they prove otherwise.5 Reports of Psychotic Episodes Soar in Great BritainNow, after some 19 months of abnormal “pandemic life,” the data are starting to reflect McDonald’s fears. For example, in the U.K., psychiatric referrals for first-time psychotic episodes have skyrocketed. As reported by The Guardian, October 17, 2021:6
Psychosis Takes a Heavy Toll on a Person’s LifeDeputy chief executive of Rethink Mental Illness, Brian Dow, commented on the findings:8
According to a spokesperson for the British Department of Health and Social Care, the agency will expand the NHS mental health services budget by £2.3 billion ($3.1 billion) per year by 2023/2024. They’ve also added £500 million ($691 million) to the 2021 budget to provide services to those hit hardest by pandemic measures.9 Anxiety and Depression Have Increased Dramatically WorldwideAnother study,10,11 looking at the rates of anxiety and depression worldwide, found both conditions increased dramatically in 2020. The researchers estimate the COVID pandemic resulted in an additional 76 million cases of anxiety and 53 million cases of major depressive disorder, over and above annual norms, with women and younger individuals being disproportionally affected. According to The Guardian:12
Lead author Damian Santomauro, Ph.D., of the University of Queensland told The Guardian:13
Increased prevalence of domestic violence may also be a contributing factor that places women at increased risk of mental problems, while young adults are more likely to become unemployed. Massive Rise in Mental Health Problems in ChildrenChildren are bearing a particularly heavy burden as adults succumb to irrational fears. It’s not surprising then that mental health referrals for children have nearly doubled in the U.K. since the start of the pandemic.14 According to British authorities, 16% of children between the ages of 5 and 16 were diagnosed with a mental disorder in 2020, compared to 10.8% in 2017.15 As noted in a September 23, 2021, press release by the Royal College of Psychiatrists:16
Eating disorders are also more prevalent than ever, and the rapid increase has left many children waiting months for treatment — delays that could have life-threatening consequences — as facilities are at capacity. The press release quotes a mother whose teenage daughter relapsed into anorexia during the pandemic:17
Mass Delusional Psychosis Traumatizes ChildrenIndeed, the widespread insanity on display among adults can have severe and lasting effects on children as they grow up. According to McDonald (see interview above), the mental states of the children he’s treated during this pandemic are far worse than he’s used to seeing in these age groups. This tells us the trauma inflicted by pandemic measures is very serious. One of the worst traumas inflicted on children has been the ridiculous idea that they might kill their parents or grandparents simply by being around them. They’re also being taught to feel guilty about behaviors that would normally be completely normal — as just one example: hysterical adults calling a toddler who refuses to wear a mask a “brat,” when resisting having a restrictive mask put across your face is perfectly normal at that age. It's extremely abnormal for children to grow up thinking that they’re a danger to people around them, and that everyone around them is a danger to them. It’s completely abnormal to grow up thinking that facemasks, gloves and physical separation are required to stay alive. Adults have also twisted irrational fear into a virtue, which is doubly tragic and wrong. Wearing a mask has become a way to demonstrate that you’re a “good person,” someone who cares about others, whereas not wearing a mask brands you as an inconsiderate lout, if not a prospective mass murderer, simply by breathing. What’s more, by encouraging us to remain in fear and allow it to control and constrain our lives, the fear has become so entrenched that anyone who says we need to be fearless and fight for our freedoms is attacked for being both stupid and dangerous. Adults Must Be Healed to Save the ChildrenIt’s adults who are mindlessly inflicting this emotional trauma on an entire generation. As noted by McDonald in his interview, a primary cause of depression among children is feeling disconnected from family and friends. Everyone, but children in particular, needs face-to-face contact, physical contact, and emotional intimacy. We need these things to feel safe around others and within our own selves. Digital interactions cannot replace these most basic human needs, and are inherently separating. McDonald cites U.S. Centers for Disease Control and Prevention statistics showing there was a 400% increase in adolescent depression during 2020 compared to the year before, and in 25% of cases, they contemplated suicide. These are unheard of statistics, he says. Never before have so many teenagers considered committing suicide. According to McDonald, parents and adults in general are to blame, because they are the ones scaring children to the point they don’t feel life is worth living anymore. This is why we can’t just treat the children. We must also address the psychosis of the adult population that is causing all this trauma. Mass Delusion Is Leading Us Into SlaveryThe mass delusion must also be addressed because it’s driving us all, sane and insane alike, toward a society devoid of all previous freedoms and civil liberties, and the corrupt individuals in charge will not voluntarily relinquish power once we’ve given it to them. Clearly, many of our political leaders know COVID-19 isn’t the deadly plague it’s been made out to be. They issue stay-at-home orders from their vacation homes in the Caribbean and repeatedly break their own mask and lockdown mandates. They ride their bikes, stroll through the park, have family gatherings and dine out without a care. They’re simply playing along, following the narrative coming from technocratic strongholds like the World Health Organization, because it benefits them. You could say the ruling class suffers from a different kind of psychosis. As explained in “Mass Psychosis — How an Entire Population Becomes Mentally Ill,” totalitarianism actually begins as psychosis within the ruling class, as the individuals within this class are easily enamored with delusions that augment their power. And no delusion is greater than the delusion that they can, and should control and dominate others. Whether the totalitarian mindset takes the form of communism, fascism or technocracy, a ruling elite that has succumbed to their own delusions of grandeur then sets about to indoctrinate the masses into their own twisted worldview. All that’s needed to accomplish that reorganization of society is the manipulation of collective feelings. Sadly, many citizens are unwittingly aiding and abetting the global power grab that will result in our enslavement. Fear fueled hysteria, which led to mass delusional psychosis and group control where citizens themselves support and press for the elimination of basic freedoms. There’s no doubt at this point that a totalitarian society is the ultimate end of this societal psychosis unless we do something about it. The truth is, we’re as safe now as we ever were. We must not allow our freedoms to be taken from us due to delusional fears. As noted by Cheah in her article:18
We Must Restore SanityOnce a society is firmly in the grip of mass psychosis, totalitarians are free to take the last, decisive step: They can offer a way out, a return to order. The price is your freedom. You must cede control of all aspects of your life to the rulers, because unless they are granted total control, they won’t be able to create the order everyone craves. This order, however, is a pathological one, devoid of all humanity. It eliminates the spontaneity that brings joy and creativity to one’s life by demanding strict conformity and blind obedience. And despite the promise of safety, a totalitarian society is inherently fearful. It is built on fear, and is maintained by it too. So, giving up your freedom for safety and a sense of order will only lead to more of the same fear and anxiety that allowed the totalitarians to gain control in the first place. Knowing this, we must remember to embrace courage, truth, honesty and freedom as we move forward — not just in our thoughts and words but also in our actions. People cannot think logically when in a state of delusional psychosis, which is why sharing information, facts, data and evidence tends to be ineffective except in cases where the person was acting out of peer pressure rather than a delusional belief. Typically, the best you can do is stand firm and act in alignment with truth and objective reality, much like you would if you were a first responder faced with an accident victim who is responding hysterically to what you know is only a minor injury. In short, to help return sanity to an insane world, you first need to center yourself and live in such a way as to provide inspiration for others to follow — speak and act in such a way as to demonstrate that you are not afraid to live life and return to normalcy. from http://articles.mercola.com/sites/articles/archive/2021/10/28/mass-psychosis-real-global-pandemic.aspx
0 Comments
In early 2020, as scientists were analyzing the SARS-CoV-2 virus, it was theorized the virulence and infectivity could be explained by gain-of-function research. Months of lab analyses and political arguments ensued over whether the virus was leaked from the lab or developed naturally in the wild. Despite public outcry and denials from top health experts that the virus was created, the preponderance of the evidence indicates the virus was manipulated in the lab.1 Then, the United States Agency for International Development (USAID), publicly announced October 5, 2021, they would grant Washington State University $125 million “to detect emerging viruses.”2 This is far greater than the $7.4 million Newsweek3 reported was granted to the NIAID for gain-of-function work on bat coronavirus in Wuhan, China. Dr. Kanta Subbarao is from the Laboratory of Infectious Disease at the National Institute of Allergy and Infectious Diseases (NIAID) at the National Institutes of Health (NIH).4 According to Subbarao, these experiments “are routine virological methods” and “emphasized that such experiments in virology are fundamental to understanding the biology, ecology and pathogenesis of viruses and added that much basic knowledge is still lacking for SARS-CoV and MERS-CoV.” Historically, the NIH had funded gain-of-function research, but this was paused in October 2014. December 19, 2017, the NIH announced they would lift the funding pause on gain-of-function research and stated:5
As Newsweek reported, the "second phase of the project, beginning that year [2019], included additional surveillance work but also gain-of-function research for the purpose of understanding how bat coronaviruses could mutate to attack humans. The project was run by EcoHealth Alliance, a nonprofit research group, under the direction of president Peter Daszak."6 After months of public and political debate, argument and division, the U.S. government agency USAID stepped into the spotlight again and awarded millions to a university “to make sure the world is better prepared.”7 University Accepts $125 Million for Gain-of-Function ResearchWashington State University published a press release8 October 5, 2021, announcing they had been awarded $125 million from USAID. Called a “cooperative agreement,” the university is heading up a new five-year global project in which they have been asked to9 “… detect and characterize unknown viruses which have the potential to spill over from wildlife and domestic animals to human populations.” The project will partner with 12 countries throughout Africa, Latin America and Asia. The idea is to carry out animal surveillance within the country’s borders using their facilities. USAID announced the project “to detect unknown viruses with pandemic potential” as part of Discovery & Exploration of Emerging Pathogens Viral Zoonoses (DEEP VZN).10 The organization believes that SARS-CoV-2 has demonstrated how infectious diseases threaten society. This is especially true of viruses that have been manipulated to increase virulence and infectivity in humans.11 The goal of the project is to collect over 800,000 samples over five years from wildlife and then determine the zoonotic potential of these viruses.12
Ebola virus was first discovered in 1976 and has since led to several deadly outbreaks in African countries. The CDC13 writes that scientists do not know where Ebola virus comes from. However, the virus can spread through direct contact with body fluids and tissues of infected animals. Nipah was first discovered in 199914 and the first outbreak resulted in 300 human cases and more than 100 deaths. The animal host is believed to be the fruit bat that can spread the disease to animals and humans. The infection also spreads from person to person and can range from mild to severe. Up to 70% of those infected between 1998 and 2018 have died. The project expects to find between 8,000 a nd 12,000 new viruses, “which researchers will then screen and sequence the genomes of the ones that pose the most risk to animal and human health.”15 In case this sounds familiar, as Breaking Points anchor emphasizes, this has been “code” for gain-of-function research,16 or detecting viruses that have not yet “emerged.” Documents Reveal Virus Was Manipulated to Increase VirulenceAn ongoing Freedom of Information Act litigation brought by The Intercept17 against the NIH resulted in the release of over 900 pages of previously undisclosed documents that detailed the work of EcoHealth Alliance as a subcontractor of gain-of-function research on bat coronavirus through the Wuhan Institute of Virology. It’s important to note that the moratorium on federal funding of gain-of-function research instituted in 2014 was initiated on the heels of a high-profile lab mishap at the CDC and controversial experiments over deadly bird flu virus that was manipulated to be more contagious.18 Reportedly, the goal was to determine if bird flu could mutate in the wild and start a pandemic. David Relman, a microbiologist from Stanford University, stated the obvious when he said,19 "I don't think it's wise or appropriate for us to create large risks that don't already exist.” The new documents released under the FOIA request by The Intercept contained previously unpublished proposals by the NIAID and updates to the EcoHealth Alliance’s research. As reported in The Intercept,20
According to The Intercept, Richard Ebright, molecular biologist at Rutgers University, also reviewed the documents released in the FOIA. He told The Intercept that the documents contained vital Information about the research being conducted in the Wuhan lab. He wrote:21
In other words, the lab was doing parallel research on two types of coronaviruses that were able to infect humanized mice. In a series of posts on Twitter, Ebright goes on to say:22
This new information again questions the origins of COVID-19, which many scientists proposed was from a wet market in China where humans and animals are in close contact. However, bioscience safety experts have long suspected a lab origin. It appears that some in the U.S. government and some scientists have not learned from the gain-of-function research in Wuhan and have brought the problem home to roost. International Athletes Willfully Exposed to Lab-Leaked VirusWhether the virus was released intentionally or accidentally is a question for another day. Long before the outbreak, scientists had expressed concerns that these kinds of experiments may end up creating the thing they were reportedly working against. As the Intercept reports,23 in 2014 a grant was awarded to EcoHealth Alliance titled “Understanding the Risk of Bat Coronavirus Emergence.” Part of the grant money was earmarked to identify and alter bat coronaviruses suspected of being able to infect humans. In the grant the writers acknowledged concerns stating, “Fieldwork involves the highest risk of exposure to SARS or other CoVs, while working in caves with high bat density overhead and the potential for fecal dust to be inhaled.”24 In the USAID announcement, the government agency gives an overview of the goals in one sentence:25 “The Biden-Harris Administration is committed to advancing global health security, international pandemic preparedness and global health resilience.” As the Breaking Points anchor in the video above says,26 “So essentially, we have learned nothing.” August 1, 2021, Rep Michael McCaul, R-Texas, the ranking member of the House Foreign Affairs committee, published an addendum to the investigation into the origins of SARS-CoV-2. The investigation concluded:27
By the end of August 2021, the White House released a statement from President Biden essentially calling the intelligence report inconclusive,28 “while this review has concluded, our efforts to understand the origins of this pandemic will not rest.” Multiple pieces of information led the committee to conclude there was ample evidence to support genetic modification of the coronavirus and there was a cover-up which “likely turned what could have been a local outbreak into a global pandemic.”29 The cover-up involved the 2019 Military Games held October 18, 2019, in Wuhan China. The report demonstrated that by October 2019, health officials in Wuhan were well aware of an outbreak of infectious disease. The athletes reported that the city appeared to be in lockdown30 while they were there. The games drew over 9,000 athletes from 109 countries. The Chinese government had 236,000 volunteers, 90 hotels, three railroad stations and more than 2,000 drivers available for the athletes. The report included a quote from a Canadian Armed Forces personnel who participated in the games, which appeared in The Financial Post.31 He was told the lockdown in the city was to make it easier for the participants in the games to get around. Twelve days after arrival in Wuhan, he was sick with fever, chills, vomiting and insomnia. He reported that on the flight home to Canada, 60 athletes were isolated at the back of the plane for the 12-hour flight with a range of symptoms including coughing and diarrhea. After returning home, the same service member found his family members got ill, which the report finds is:32
Funding Gain-of-Function Research Out in the OpenFollowing the release of The Intercept report and additional grant documentation, some GOP members are calling for Dr. Anthony Fauci to resign while others want him fired from his position on the White House COVID-19 response team.33 U.S. Sen. Rand Paul, R-Ky.., has referred Fauci to the Department of Justice for an investigation for possible perjury charges relating to his Congressional testimony in May 202134 and July 2021,35 when he vehemently denied ever having funded gain-of-function research. Paul specifically asked the DOJ36 to investigate whether Fauci violated 18 U.S. Code § 10012137 — which makes it a federal crime to make “any materially false, fictitious or fraudulent statement or representation” as part of “any investigation or review" conducted by Congress — or any other statute. How much genetic manipulation and gain-of-function research that occurs as a result of the $125 million grant to the university may not come to light for years. However, it is incumbent on our government to ensure biosafety in the labs doing the research and, for the public, to call for a halt of this type of research that “create[s] large risks that don’t already exist.”38 from http://articles.mercola.com/sites/articles/archive/2021/10/27/125-million-poured-into-gof-lab-leak-research.aspx This article was previously published January 20, 2021, and has been updated with new information. While vitamins C and D have garnered much attention in the fight against COVID-19, B vitamins can also play an important role, according to two recent papers — niacin (B3) in particular. The first, "Be Well: A Potential Role for Vitamin B in COVID-19,"1,2 was published in the February 2021 issue of the journal Maturitas. The paper is the result of a joint collaboration between researchers at the University of Oxford, United Arab Emirates University and the University of Melbourne, Australia. While no studies using B vitamins have been performed on COVID-19 patients, the researchers stress that, based on B vitamins' effects on your immune system, immune-competence and red blood cells (which help fight infection), supplementation may be a useful adjunct to other prevention and treatment strategies. As noted by the authors:3
B Vitamins Play Many Roles in COVID-19 Disease ProcessImportantly, B vitamins can influence several COVID-19-specific disease processes, including:4
The paper goes on to detail how each of the B vitamins can help manage various COVID-19 symptoms:5
Niacin — A Missing Piece of the COVID-19 Puzzle?The second paper,12 "Sufficient Niacin Supply: The Missing Puzzle Piece to COVID-19 and Beyond?" (which is a preprint and has yet to undergo peer review), focuses specifically on niacin (B3), raising the question of whether this vitamin might actually be a crucial player in the COVID-19 disease process. As noted in the abstract:
As noted in this paper, a primary hallmark of COVID-19 pathology is the cytokine storm, which can lead to multiple organ failure and death. Marked elevations in proinflammatory cytokines are to blame for this chain of events, most notable of which are interleukin-6 (IL-6), interleukin-1β (IL-1β), tumor necrosis factor-α (TNF-α) and monocyte chemoattractant protein-1 (MCP-1). If you can decrease and control these damaging cytokines, you stand a good chance of thwarting the cytokine storm and the downstream damage it causes. Nicotinamide adenine dinucleotide (NAD+) plays an important role in this, and niacin is a building block of NAD. As explained in "Be Well: A Potential Role for Vitamin D in COVID-19":13
Aside from markedly decreasing proinflammatory cytokines, niacin has also been shown to:14
Niacin Modulates the Bradykinin StormCOVID-19 also triggers bradykinin storms. Bradykinin is a chemical that helps regulate your blood pressure and is controlled by your renin-angiotensin system (RAS). The bradykinin hypothesis provides a model that helps explain some of the more unusual symptoms of COVID-19, including its bizarre effects on your cardiovascular system. Researchers have discovered SARS-CoV-2 downregulates your body's ability to degrade or break down bradykinin. The end result is a bradykinin storm, and this appears to be an important factor in many of COVID-19's lethal effects, perhaps even more so than the cytokine storms associated with the disease. As bradykinin accumulates, the more serious COVID-19 symptoms appear. Vitamin D has a significant impact on the RAS,15 and can therefore help prevent a bradykinin storm, but niacin also plays an important role. As noted in "Sufficient Niacin Supply: The Missing Puzzle Piece to COVID-19 and Beyond?":16
The paper also expounds on the role of NAD+, and why niacin is a useful strategy for boosting NAD+:18
Recommended UseThe paper19 goes deep into the biochemical aspects of how niacin works in your body, so if you're interested in that, you may want to read through it. In summary, as it pertains to COVID-19, the important thing to understand is that there appears to be a causative link between low niacin status and SARS-CoV-2 infection. According to the authors, SARS-CoV-2's ability to invade your body is dependent on whether calcium signaling can properly proceed, which in turn is dependent on the presence of NAADP. And, as explained in the quoted section above, niacin forms NAADP in your body. NAADP-dependent calcium signaling is responsible both for the inhibition of viral entry into cells and driving the virus out of already infected cells. And, again, the authors stress that "nothing outside of sufficiently, dynamically supplied niacin is capable of readily leading to the NAADP supply needed in these acidic environments for therapeutic action that counteracts inflammatory disease progression." They also point out that the flushing you get from niacin is part of how the niacin drives inflammatory free radicals out of the cells. As you continue to take the supplement at a consistent, sufficiently high dose, that flushing will gradually lessen, which is a sign that your body is reaching a healthy homeostasis.
While the flushing can be uncomfortable, the authors stress that it is "indeed safe," and actually "should be sought when needed for its anti-inflammatory properties." Suggested DosingAs a "health restorative therapy" for those diagnosed with SARS-CoV-2, they recommend starting with a dose of 500 milligrams of immediate-release niacin, two to three times a day, ideally within the first 48 hours of symptom onset. As your flush response lessens, increase your dose to 1,000 mg, two to three times a day.21
Although the authors suggest you can use niacin prophylactically, using that same dose, I disagree. According to the authors:23
There may be some value to the high doses in acute COVID-19 infections but I am skeptical. I am a huge fan of NAD+ augmentation and have been using it for years. My research suggests you really only need about 25 mg per day of niacin, which will not cause flushing in nearly anyone. I believe most would benefit from taking 25 mg of niacin daily, preferably in a well-balanced B complex, which would have thiamine (B1) that has also been shown to be useful in COVID-19. Other alternatives to high-dose niacin would be nicotinamide riboside (NR) and nicotinamide mononucleotide (NMN), which is my personal favorite. I believe that compounding these into rectal suppositories would avoid most of the methylation of the supplement and supply you with higher NAD+ tissue levels. Another downside of high-dose niacin is that it breaks down to nicotinamide and in high doses, nicotinamide will inhibit Sirt1, which is an important longevity protein. Personally, I believe a superior strategy to high-dose niacin in acute COVID-19 would be to use nebulized hydrogen peroxide at 0.1%. I have never seen or heard of this intervention failing in the treatment of COVID-19. 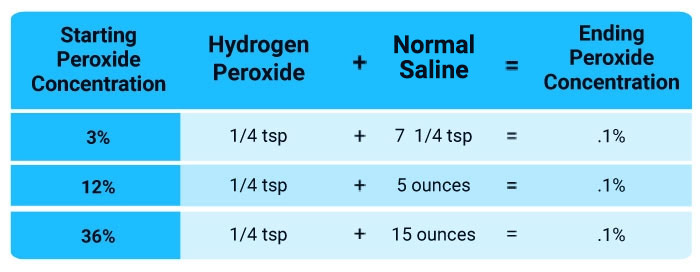 How to Improve Your Vitamin B StatusAs a general rule, I recommend getting most if not all of your nutrition from real food. This will work well for most B vitamins, but not if you're using niacin therapeutically, as described above. For that, you will need to take a supplement. That said, the list below will show you which foods contain which B vitamins, as well as provide general guidance on dosage if you're taking a supplement. If you're trying to improve your vitamin B status, also consider limiting sugar and eating more fermented foods. The reason for this is because the entire B group vitamin series is produced within your gut, assuming you have healthy gut flora. Eating real food, including plenty of leafy greens and fermented foods, will provide your microbiome with important fiber and beneficial bacteria to help optimize your internal vitamin B production.
from http://articles.mercola.com/sites/articles/archive/2021/10/27/what-are-the-benefits-of-niacin.aspx Diabetes has reached crisis levels in the U.S., with 10.5% of Americans affected.1 That data came from 2018 — before the pandemic — and the problem has only worsened since. Diabetes was the seventh leading cause of death in the U.S. in 2017,2 but diabetes deaths surged during the COVID-19 pandemic, rising 17% in 2020.3 While COVID-19 was a problem — 39.5% of COVID-19 deaths occurred among people with diabetes4 — even diabetics who didn’t get COVID-19 suffered, often falling victim to isolation, social distancing, lack of medical care and fear, instead. Younger people have been disproportionately affected, with diabetes deaths among 25- to 44-year-olds jumping 29% in 2020. Other deaths from everything, excluding COVID-19, rose 6% that year,5 highlighting the dismal public health failure that accelerated the diabetes pandemic. Medical System, Dietary Advice Failing People With DiabetesEven prior to the pandemic, diabetes was on an alarming trajectory that saw hospitalization for hyperglycemic crises increase by 73% from 2009 to 2015. Diabetes deaths rose by 55% during that time.6 Inactivity and poor diet are fueling the diabetes crisis, causing people to develop the condition at younger ages. Diets focused on ultraprocessed foods and fast foods are the root of the problem, as they’re loaded with seed oils — misleadingly known as “vegetable oils” — that contain toxic oxidized omega-6 linoleic acid (LA) that accelerate metabolic dysfunction.7 Yet, the American Diabetes Association continues to recommend seed oils like canola as “part of a healthy, balanced diet.”8 Diabetes is a manageable — and often reversible — condition, provided you make positive lifestyle changes and get proper medical care and advice. However, many people are limited by their insurance plans as to which care providers they can see, and others forgo medical care entirely to avoid having to pay out-of-pocket costs. As it stands, diabetes treatment costs top $230 billion a year in the U.S., yet the diabetes mortality rate is 42% higher than it is in 10 other industrialized countries.9 “The focus in U.S. health care on treating crises over preventing them doesn’t help, downplaying the importance of lifestyle changes that could lessen the severity of the disease,” a Reuters investigation reported. “‘Over and over again, the problem is worse in young adults, and there isn’t improvement in older adults,’ Ed Gregg, a former CDC researcher, told Reuters. ‘The magnitude of the increase has set us back 15 to 20 years.’”10 In fact, in 2020 only accidents and overdose deaths rose faster than diabetes deaths, which beat out Alzheimer’s disease, flu and pneumonia, stroke, heart disease, kidney disease and cancer for the dubious title of fastest-rising deaths.11 Fearful of COVID, People Died of Diabetes InsteadThe Reuters investigation follows the case of a 42-year-old woman whose death from complications of Type 2 diabetes during the pandemic was the result of isolation and fear. Locked down in her home, fearful of COVID-19, she ordered fast food and lost the motivation to eat better and exercise, and had difficulty getting adequate medical care. Ultimately, “the isolation and the financial and logistical issues proved overwhelming.”12 In another case, a 68-year-old man with Type 2 diabetes had his leg amputated after avoiding medical care for a chronic sore out of fear of COVID-19. These stories aren’t unique. Sandra Arevalo, director of community and patient education at Montefiore Hospital in Nyack, New York, told Reuters that diabetes deaths, amputations and intensive care admissions had plagued several patients she knew of after they delayed medical care during the pandemic. “The diagnosis was uncontrolled diabetes, but it was caused by COVID fear. COVID caused more damage than we realized,” Arevalo said13 Giuseppina Imperatore, with the CDC’s Division of Diabetes Translation, also told Reuters that “the impact of the COVID pandemic on people with diabetes cannot be overstated.”14 Diabetes Cases Tripled Among Youth in 2020Young people are also suffering. Among 8- to 20-year-olds, Type 2 diabetes diagnoses tripled in 2020 at Children’s National Hospital in Washington, D.C., and they’re showing up sicker than they did in the past, with 23% affected by diabetic ketoacidosis, compared to 4% in 2019.15 School closures and reduced physical activity triggered by the pandemic were likely factors in the sudden rise. “It was really pointing us to the indirect effect of social distancing,” Dr. Brynn Marks, a pediatric endocrinologist at Children’s National, told Reuters.16 Weight gain has been another consequence, with significant increases in the rate of body mass index (BMI) change noted during the pandemic among 2- to 19-year-olds, according to the CDC. The CDC noted:17
Translated into the resulting weight gain, the figures reveal that 22% of children and teens were obese in 2020,18 up from 19% in 2019. Average annual weight gain among healthy weight children was 3.4 pounds prior to the pandemic, which rose to 5.4 pounds in 2020. Among children who were already obese, the acceleration was even greater. For moderately obese children, expected annual weight gain rose from 6.5 pounds in 2019 to 12 pounds in 2020, while severely obese children’s expected annual weight gain increased from 8.8 pounds to 14.6 pounds during the pandemic. The Pandemic Made Obesity WorseAmericans are also facing an obesity crisis, which goes hand in hand with the diabetes crisis. The latest figures from the CDC state that 42.4% of Americans were obese in 2017 to 2018, an increase from 30.5% in 1999 to 2000.19 The pandemic has made these numbers even worse, as 42% of U.S. adults who responded to the American Psychological Association’s 2021 Stress in America poll said they had gained more weight than they intended since the pandemic started.20 The average weight gain among this group was 29 pounds, with 10% stating they gained more than 50 pounds during the pandemic.21 The CDC also announced September 15, 2021, that the number of states with high obesity prevalence — defined as at least 35% of residents with obesity — has nearly doubled since 2018.22 There are now 16 states where at least 35% of the residents are obese, up from nine states in 2018 and 12 in 2019. “These and other emerging data show that the COVID-19 pandemic changed eating habits, worsened levels of food insecurity, created obstacles to physical activity, and heightened stress, all exacerbating the decadeslong pattern of obesity in America,” Trust for America’s Health reported.23 Experts: ‘Quarantine’ From Ultraprocessed FoodsEliminating ultraprocessed foods is an essential part of tackling both obesity and Type 2 diabetes, as it lowers your intake of toxic seed oils. Dr. Chris Knobbe, an ophthalmologist and the founder and president of the Cure AMD Foundation, explained the complex process behind seed oils’ toxicity in his presentation at the ALLDOCS annual 2020 meeting:24
While the CDC and other health officials aren’t sounding the alarm about the risks posed by ultraprocessed foods and other toxic exposures, the scientific community is taking note. As noted by a team of researchers in the journal Food and Chemical Toxicology, the role of toxic substance exposures, which includes ultraprocessed foods and poor diet, is underreported in the COVID-19 pandemic.25 “In short, it is the pervasive, constant exposure to toxic stressors in our environment, in combination with genetic factors, that cause us to develop diseases that impair our immune systems and make us susceptible to serious COVID-19 infection,” reported the Alliance for Natural Health.26 As the researchers noted, this includes lifestyle factors such as inactivity, smoking, excessive alcohol consumption, poor diet including ultraprocessed foods and refined grains and chronic sleep deprivation — all factors that also affect your weight and risk of diabetes.27 In order to protect the public, a “quarantine” from toxins like ultraprocessed foods, environmental chemicals and more would be far more effective than quarantining from one virus,28 and for long-term pandemic prevention, the researchers believe, and I would strongly agree, that such toxicology-based approaches should be given priority over virology-based approaches.29 Healthy Lifestyle for Type 2 Diabetes PreventionMany aspects of the COVID-19 pandemic response, from lockdowns to school closures, have worsened the already perilous diabetes and obesity epidemics, but you can take action to protect your health. In addition to eliminating ultraprocessed foods — including fast foods and most restaurant foods — from your diet, give intermittent fasting a try. Time restricted eating (TRE) is a simple powerful intervention that mimics the eating habits of our ancestors and restores your body to a more natural state that allows a whole host of metabolic benefits to occur.30 TRE involves limiting your eating window to six to eight hours per day instead of the more than 12-hour window most use. Research shows, for instance, that TRE promotes insulin sensitivity and improves blood sugar management by increasing insulin-mediated glucose uptake rates,31 which is important for resolving Type 2 diabetes. In another study, when 15 men at risk of Type 2 diabetes restricted their eating to even a nine-hour window, they lowered their mean fasting glucose, regardless of when the “eating window” commenced.32 Remember when you eat is also important. I recommend adopting a cyclical ketogenic diet, which involves radically limiting carbs (replacing them with healthy fats and moderate amounts of protein) until you’re close to or at your ideal weight, ultimately allowing your body to burn fat — not carbohydrates — as its primary fuel. And always remember the most dangerous foods in your diet are seed oils, commonly hidden in all chicken, pork, salad dressings and any sauces or dressings at a restaurant. from http://articles.mercola.com/sites/articles/archive/2021/10/27/diabetes-pandemic.aspx Your kidneys are essential to filter excess water and waste from your blood.1 Chronic kidney disease (CKD) can lead to dialysis and the need for a kidney transplant to live. One woman in Colorado recently learned that the University of Colorado Health System's policy change meant she was no longer eligible for a kidney transplant.2 Conditions that damage your kidney and decrease their function are called chronic kidney disease.3 Chronic kidney disease is divided into stages.4 The higher the stage, the greater the damage to the kidneys. Stages range from Stage 1 indicating mild kidney damage to Stage 5, which is just before complete failure. Dialysis is needed when a person reaches Stage 5 kidney failure.5 This process helps the body eliminate waste products, salt and extra water, and helps control blood pressure. Dialysis is done in a dialysis unit or at home, depending upon the process used. However, without a kidney transplant, the average life expectancy on dialysis is between five and 10 years. For the majority of people, a kidney transplant is the best option. Although it is not a cure for kidney disease, it can improve the quality and length of life.6 The United Network for Organ Sharing (UNOS) maintains the list of individuals who need any type of organ transplant, including a kidney transplant. On average, people wait three to five years for a kidney transplant. In some areas, it can be even longer. The wait time is dependent on blood type and history of blood transfusions or transplants. Leilani Lutali's situation became public when Colorado state Rep. Tim Geitner published the letter that Lutali received from UCHealth denying the transplant. Geitner posted a copy of the letter on Twitter without Lutali's identifying information saying, "UCHealth denies lifesaving treatment — kidney transplant — to El Paso County resident. See my FB live post @timgeitnercolorado"7 Unvaccinated Woman Denied Direct Kidney TransplantLutali met her kidney donor, Jaimee Fougner, at a Bible study. In August 2021, Lutali confirmed with UCHealth that a COVID shot was not required, but by September 28, 2021, she learned she would be denied the lifesaving transplant because she and her donor were unwilling to get the shot. In an interview with CBS,8 we learn that Lutali has already had COVID and Fougner cannot get the shot for religious reasons, in what the news anchor called the "latest example of someone facing severe consequences after refusing to get vaccinated for COVID." Despite thousands of deaths and disabilities9 resulting from the vaccine, another newscaster quoted UCHealth, saying,10 "The hospital system says that keeping people from dying unnecessarily is kind of the point." Hospitals have routinely placed conditions on organ transplants, hoping to extend the life of those who receive the organ. Some of these requirements include stopping smoking, avoiding alcohol, changing eating habits or taking certain vaccinations.11 However, with the COVID shot, Lutali clearly expresses her concern that it's still new and there are many questions about how it would affect her health.12 Interestingly, the hospital also requires the donor to be vaccinated. They reason that a living donor could pass a COVID infection to the recipient after testing negative.13 And yet, according to government officials, anyone vaccinated can pass COVID to anyone else.14 Therefore, using the hospital's reasoning, it does not track that the donor must also be vaccinated. Lutali is receiving a direct donation and is not taking a kidney from the transplant waiting list. According to the Department of Health Resources and Services Administration,15 there are currently 106,729 people on the waiting list and 17 people will die every day waiting for an organ transplant. It is worth noting that while government officials and hospitals continue to call the shot a vaccine, it does not meet the definition of a vaccine by the CDC before 2021. Until September 1, 2021, the definition was:16
However, just days after the FDA approved the Pfizer shot,17 September 1, 2021, the CDC changed the definition of a "vaccine" to:18
As you may have noticed, in this latest iteration, a vaccine is a "preparation" that:
Data Show Transplant Deaths Related to Comorbid Conditions9 News reported that the hospital released a statement saying,19 "… studies indicate the mortality rate for transplant recipients who test positive for COVID ranges from 18% to 32%, compared to a 1.6% mortality rate among all people who have tested positive." After a kidney transplant, patients must take anti-rejection drugs that have a significant impact on their innate immune system.20 Children and adults are prescribed a combination of immunosuppressant medications that must be taken for as long as the kidney transplant is working. These drugs have serious side effects, including an increased risk for all infections.21 They also increase the risk for influenza infection. However, while past research has demonstrated influenza vaccination may reduce the risk of flu after a kidney transplant,22,23,24 UCHealth has not mandated a flu vaccine, only a COVID shot. One literature review25 found the overall mortality rate from COVID-19 was 20% for those who had received a transplant. However, the median age range of the patients was 66 years and the participants had other comorbid conditions often related to severe disease, including high blood pressure, diabetes, malignancy and chronic obstructive pulmonary disease. In one prospective cohort study26 in France, 5% of the participants were diagnosed with COVID. Again, the mortality rate was 24% with comorbidities that included obesity, diabetes, asthma and chronic pulmonary disease. A third study27 enrolled 1,073 patients with a mean age of 60 years who had either a kidney transplant or were on dialysis. Mortality was associated with older age in transplant patients, and with age and frailty in those on dialysis. Interestingly, one study28 found factors strongly associated with mortality from COVID after a kidney transplant were demographic, clinical and social determinants, such as age, sex, body mass index, diabetes, education and socioeconomic status. Religious Exemption Based on Use of Aborted Fetal CellsFougner cannot get the shot for religious reasons, supported by the announcement in February 2021 by the New Orleans Archdiocese in which they stated the Johnson & Johnson vaccine was "morally compromised as it uses the abortion-derived cell line in development and production of the vaccine as well as the testing." While the Archdiocese recommended avoiding the Johnson & Johnson vaccine, it did not have the same concerns for Pfizer and Moderna. However, other clergy disagree since abortion-derived cell lines were used in lab testing for all the vaccines. This debate has a long history that centers on using HEK293 cells that were harvested from an aborted fetus in the early 1970s.29 This is the moral dilemma that is at the basis for most religious exemptions for the vaccine. Several fact-checkers including PolitiFact,30 The Associated Press31 and Snopes32 have labeled this claim as false because the fetal cells are not directly in the vaccine. However, as it turns out the fact-checkers relied on semantics when, technically, fetal cells are used during the production of certain vaccines. Several of the cell lines commonly used in vaccine development that originated from aborted fetuses include:
Some critics of abortion-derived cell lines have claimed that since the vaccines literally do not contain abortion-derived cells, the entire claim is false. In other instances, fact-checkers claim the cell lines are not original, as in the statement made in an archived article from The Washington Post,37 but rather a clone. However, the claim that the cells are clones of the original is like saying your 20-year-old or 40-year-old body is no longer your body since all the cells are copies of those when you were a baby. They are, in essence, a clone of the original. Yet, there is virtually no difference between cells that grow and multiply in a petri dish and those that grow and multiply in your body during your lifetime. If the cells in your body are still you, then the cells in the petri dish are still those of the original aborted fetus. It has become apparent that fact-checkers are trying to dissuade people from having a public conversation about the ethics of using abortion-derived cell lines to produce and test vaccines. How Many Deaths Attributed to Disease or Lack of Treatment?So how many deaths could there be that are attributable to disease or lack of treatment? The answer to this question is unknowable. At the start of 2020, doctors scrambled to find treatments that would be effective against the SARS-CoV-2 virus. If you have been reading my newsletter, you know that I have interviewed several of these experts, including Dr. Vladimir Zelenko,38,39 who has been successfully treating his patient population with hydroxychloroquine and zinc. In the video above you can see Dr. Peter McCullough's early treatment regimen at minute 53:40 that includes a nutraceutical bundle, progressing to monoclonal antibody therapy, antiinfectives like hydroxychloroquine or ivermectin, antibiotics, steroids and blood thinners. You have also heard from Front Line care doctors, including Dr. Paul Marik who is a critical care doctor at Sentara Norfolk General Hospital in East Virginia. Marik was one of the founding critical care doctors who formed the Front Line COVID-19 Critical Care Working Group (FLCCC)40 early in the pandemic. In each case, the experiences of these physicians have demonstrated treatment protocols that have severely reduced the mortality rate in those treated. Yet, physicians who chose to use these protocols or institute early treatment for their patients experienced the unthinkable — they were being threatened with the loss of their medical license for trying to help.41,42 Hospitals were sued to use ivermectin, and the decisions were reversed.43 Without hope of early or effective treatment, the public was being conditioned to wait for a vaccination. Since the U.S. rollout of the vaccine in December 2020,44 through October 1, 2021, the Vaccine Adverse Event Reporting System45 has recorded:
Approved Drugs May Be DeadlyInstead of using drugs with a low side effect profile, the FDA46 approved the use of remdesivir October 22, 2020. Remdesivir is an antiviral drug that's a nucleoside/nucleotide reverse transcriptase inhibitor. According to the National Institutes of Health,47 the drug is approved for hospitalized adult and pediatric patients 12 years and older and has emergency use authorization for hospitalized pediatric patients younger than 12 years. This treatment protocol is not recommended by the World Health Organization that published a conditional recommendation against remdesivir November 20, 2020, which they have not rescinded.48 They stated, "there is currently no evidence that remdesivir improves survival and other outcomes in these patients."49 What is important to note is that remdesivir, the only recommended treatment protocol in the U.S., has significantly damaged kidney function in past studies50,51 and has not been used yet in COVID vaccine clinical trials for patients with kidney damage.52 I recommend that you proactively work to support your immune system using strategies evidence has demonstrated reduces your risk of severe disease. Should you get sick at home, there are several early treatment protocols you may consider that do not require prescription. If you have had an organ transplant or other underlying medical condition, check with your health care professional, or a physician familiar with early treatments and your health condition. You may find a list of telemedicine doctors at Aesthetic Advisor53 or the FLCCC.54 Take care to share your current medical history and ensure the drugs being prescribed are safe for your situation. from http://articles.mercola.com/sites/articles/archive/2021/10/26/all-organ-donors-and-recipients-must-be-vaccinated.aspx It was only a matter of time before a vaccine-resistant strain of COVID-19 would surface, and that time has already come to pass. As reported by The Conservative Treehouse October 3, 2021:1
Vaccine-Evading Variants Are EmergingThe study, posted on the preprint server medRxiv, August 25, 2021, concluded that those who are fully “vaccinated” against COVID-19 are in fact more susceptible to COVID variant infections than unvaccinated people. Vanden Bossche’s theory was that vaccine antibodies would suppress natural antibody responses, allowing variants to slip through, and this seems to be what’s happening. As explained by The Conservative Treehouse October 3, 2021:4
According to the authors of the study:5
“Be careful around vaccinated people, because they can carry a more resistant form of COVID-19,” The Conservative Treehouse warns, adding that the narrow protection you get from the COVID shot will inevitably necessitate a booster shot for each emerging new variant that is resistant to the shots. UK Data Show Increased COVID Mortality Among Fully VaxxedBritish data also raise serious questions about the wisdom of this injection campaign. In its Technical Briefing 23,6 published September 17, 2021, Public Health England reveals data showing the COVID death toll is actually higher among the fully vaccinated compared to the unvaccinated. Between February 1, 2021, and September 12, 2021, 157,400 fully vaccinated patients (26.52% of total cases) were diagnosed with a Delta variant. Among the unvaccinated, there were 257,357 Delta variant cases (43.36% of total cases). However, while Delta infections were far more prevalent among the unvaccinated, these patients also had better outcomes. In all, 63.5% of those who died from COVID-19 within 28 days of a positive test were fully vaccinated (1,613 compared to 722 in the unvaccinated group). More Signs of Antibody-Dependent EnhancementIn a letter to the editor of the Journal of Infection,7 published August 9, 2021, three researchers point out that “infection-enhancing anti-SARS-CoV-2 antibodies recognize both the original Wuhan/D614G strain and Delta variants,” which suggests antibody-dependent enhancement (ADE) is emerging. According to the authors:8
As noted by independent journalist Sharyl Attkisson,9 “Despite the fact that multiple medical authorities predicted, told us, and hoped, ADE would not impact Covid-19 vaccines, data from the study indicates it has done just that.” Antibody Levels Decrease After Second DoseWhile you’re not considered “fully vaccinated” until 14 days after your first dose of Janssen’s or AstraZeneca’s shot, or second dose of Moderna’s or Pfizer’s, a recent Israeli study found antibody levels actually decrease after the second dose of Pfizer’s COVID shot. The findings were reported by The Jerusalem Post, October 7, 2021:10
In all, 4,868 staff members at the Sheba Medical Center participated in the study,12 undergoing monthly serological tests to measure their antibodies for up to six months after their second Pfizer shot. Everyone, regardless of age or gender, saw a rapid decline in their antibodies after the second dose. IgG antibodies — which are part of your humoral immune response — decreased at a consistent rate over time, whereas the neutralizing antibodies rapidly decreased during the first three months, and then slowed down thereafter. According to the authors:13
COVID-19 Unrelated to Jab in 68 Countries, 2,947 US CountiesThe Israeli findings above can help explain the findings of a study14 published September 30, 2021, in the European Journal of Epidemiology, which found no relationship between COVID-19 cases and levels of vaccination in 68 countries worldwide and 2,947 counties in the U.S. If anything, areas with high vaccination rates had slightly higher incidences of COVID-19. According to the authors:15
Iceland and Portugal, for example, where more than 75% of their populations are fully vaccinated, had more COVID-19 cases per 1 million people than Vietnam and South Africa, where only about 10% of the populations are fully vaccinated.16 Data from U.S. counties showed the same thing. New COVID-19 cases per 100,000 people were “largely similar,” regardless of the percentage of a state’s population that was fully vaccinated. “There … appears to be no significant signaling of COVID-19 cases decreasing with higher percentages of population fully vaccinated,” the authors wrote.17 Notably, out of the five U.S. counties with the highest vaccination rates — ranging from 84.3% to 99.9% fully vaccinated — four of them were on the U.S. Centers for Disease Control and Prevention’s “high transmission” list. Meanwhile, 26.3% of the 57 counties with “low transmission” have vaccination rates below 20%. The study even accounted for a one-month lag time that could occur among the fully vaccinated, since it’s said that it takes two weeks after the final dose for “full immunity” to occur. Still, “no discernable association between COVID-19 cases and levels of fully vaccinated” was observed.18 Key Reasons Why Reliance on Jabs Should Be ReexaminedThe study summed up several reasons why the “sole reliance on vaccination as a primary strategy to mitigate COVID-19” should be reevaluated. For starters, the jab’s effectiveness is rapidly waning. “A substantial decline in immunity from mRNA vaccines six months’ post immunization has … been reported,” the researchers noted, adding that even severe hospitalization and death from COVID-19, which the jabs claim to protect against, have increased from 0.01% to 9% and 0% to 15.1%, respectively, among the fully vaccinated from January 2021 to May 2021.19 If the jabs work as advertised, why haven’t these rates continued to rise instead of fall? “It is also emerging,” the researchers noted, “that immunity derived from the Pfizer-BioNTech vaccine may not be as strong as immunity acquired through recovery from the COVID-19 virus.”20 For instance, a retrospective observational study published August 25, 2021, revealed that natural immunity is superior to immunity from COVID-19 jabs. According to the authors:21
Reinfection Is Very RareThe fact is, while breakthrough cases continue among those who have gotten one or more COVID-19 injections, it’s extremely rare to get COVID-19 after you’ve recovered from the infection. How rare? Researchers from Ireland conducted a systematic review including 615,777 people who had recovered from COVID-19, with a maximum duration of follow-up of more than 10 months.22 “Reinfection was an uncommon event,” they noted, “with no study reporting an increase in the risk of reinfection over time.” The absolute reinfection rate ranged from 0% to 1.1%, while the median reinfection rate was just 0.27%.23,24,25 Another study revealed similarly reassuring results. It followed 43,044 SARS-CoV-2 antibody-positive people for up to 35 weeks, and only 0.7% were reinfected. When genome sequencing was applied to estimate population-level risk of reinfection, the risk was estimated at 0.1%.26 There was no indication of waning immunity over seven months of follow-up, unlike with the COVID-19 injection, which led the researchers to conclude that “Reinfection is rare. Natural infection appears to elicit strong protection against reinfection with an efficacy >90% for at least seven months.”27 All Risk for No Reward?The purpose of informed consent is to give people all of the data related to a medical procedure so they can make an educated decision before consenting. In the case of COVID-19 injections, such data initially weren’t available, given their emergency authorization, and as concerning side effects became apparent, attempts to share them publicly were suppressed. In August 2021, a large study from Israel28 revealed that the Pfizer COVID-19 mRNA jab is associated with a threefold increased risk of myocarditis,29 leading to the condition at a rate of one to five events per 100,000 persons.30 Other elevated risks were also identified following the COVID-19 jab, including lymphadenopathy (swollen lymph nodes), appendicitis and herpes zoster infection.31 Dr. Peter McCullough, an internist, cardiologist and epidemiologist, is among those who have warned that COVID-19 injections are not only failing but putting lives at risk.32 According to McCullough, by January 22, 2021, there had been 186 deaths reported to the Vaccine Adverse Event Reporting System (VAERS) database following COVID-19 injection — more than enough to reach the mortality signal of concern to stop the program. “With a program this size, anything over 150 deaths would be an alarm signal,” he said. The U.S. “hit 186 deaths with only 27 million Americans jabbed.” McCullough believes if the proper safety boards had been in place, the COVID-19 jab program would have been shut down in February 2021 based on safety and risk of death.33 Now, with data showing no difference in rates of COVID-19 cases among the vaxxed and unvaxxed, it appears more and more likely that the injections have a high level of risk with very little reward, especially among certain populations, like youth. Mass Vaccination Drives MutationsIt’s well-known that if you put living organisms like bacteria or viruses under pressure, via antibiotics, antibodies or chemotherapeutics, for example, but don’t kill them off completely, you can inadvertently encourage their mutation into more virulent strains. Those that escape your immune system end up surviving and selecting mutations to ensure their further survival. Many have warned about immune escape due to the pressure being placed upon the COVID-19 virus during mass vaccination,34 and according to one mathematical model,35 a worst-case scenario can develop when a large percentage of a population is vaccinated but viral transmission remains high, such as it is now. This is a prime scenario for the development of resistant mutant strains.36 At this point, COVID-19 injection failures and serious jab-related health risks are both apparent. We now also have data showing that having a high vaccination rate does nothing to lower COVID-19 incidence. It might actually increase it slightly, as we’re seeing in India. In Kerala, India, which boasts a 93% vaccination rate, more than half of all new COVID cases are fully vaccinated, as are 57% of COVID-related deaths.37 With all data pointing in the same direction, it’s clear that COVID shots aren’t the answer. As noted in the European of Journal of Epidemiology:38
If You’re ‘Vaccinated’ You May Be High-Risk for COVIDAs predicted from the very beginning of the mass vaccination campaign, we’re now starting to see evidence of ADE, which makes people more prone to serious illness rather than less. Even if your risk for ADE is small (and we have no data on prevalence as of yet), the data we do have suggest the shots aren’t ending outbreaks, and indeed can’t, end them, as it’s the vaccinated who are facilitating the emergence of vaccine-evading variants. The real answer is natural herd immunity, as natural immunity protects against most variants and not just one. To be on the safe side, I recommend considering yourself “high-risk” for severe COVID if you’ve received one or more shots, and implement known effective treatment at the first sign of a respiratory infection. Options include the Zelenko protocol,39 the MATH+ protocols40 and nebulized hydrogen peroxide, as detailed in Dr. David Brownstein’s case paper41 and Dr. Thomas Levy’s free e-book, “Rapid Virus Recovery.” Whichever treatment protocol you use, make sure you begin treatment as soon as possible, ideally at first onset of symptoms. from http://articles.mercola.com/sites/articles/archive/2021/10/26/leaky-vaccine-breakthrough-variant.aspx This article was previously published December 07, 2021, and has been updated with new information. There's good news for those of you who have taken the proactive step to make sure your vitamin D level is optimized. Several recent studies demonstrate vitamin D can have a significantly beneficial impact on your cancer risk, both in terms of preventing cancer and in the treatment of cancer. Vitamin D Reduces Cancer MortalityIn the first of these studies,1,2 which included 25,871 patients, vitamin D supplementation was found to reduce the risk for metastatic cancer and death by 17%. The risk was reduced by as much as 38% among those who also maintained a healthy weight. This was a really poorly done study as they only gave participants 2,000 IUs a day and never measured their blood levels. Had there been no improvement, I would not have been surprised, but the fact is it still reduced metastatic cancer and death by 17%, and they found significant benefit among those who were not obese. This is pretty extraordinary but not as good as epidemiological studies that show a 50% to even 78% reduction in vitamin D-sufficient people, as suggested in a study further below. That said, UPI reported the results saying:3
The study, published in JAMA Network Open, is a secondary analysis of the VITAL Study4 which, in part, sought to determine whether taking 2,000 IUs of vitamin D per day would reduce the risk of cancer, heart disease or stroke in people who did not have a prior history of these diseases. The VITAL study itself, which followed patients for an average of 5.3 years, found no statistical difference in overall cancer rates among those who took vitamin D3, but there was a reduction in cancer-related deaths, which is what prompted this secondary analysis. Obesity May Inhibit Vitamin D's BenefitsThe fact that patients with a healthy weight derived a much greater benefit — a 38% reduced risk for metastatic cancer and death compared to 17% overall — suggests your body weight may play a significant role in whether vitamin D supplementation will provide you with the anticancer benefits you seek. According to study co-author Dr. Paulette Chandler, assistant professor of medicine at Brigham and Women's Hospital in Boston, "Our study highlights that obesity may confer resistance to vitamin D effects."5 There may be something to that. Research6 published in 2010 found that dietary fructose inhibits intestinal calcium absorption, thereby inducing vitamin D insufficiency in people with chronic kidney disease. That said, vitamin D tends to be lower in obese people in general, for the fact that it's a fat-soluble nutrient and when you're obese, the vitamin D ends up being "volumetrically diluted." As explained in the paper "Vitamin D in Obesity," published in 2017:7
While that particular paper stresses that lower vitamin D in obese individuals might not mean that they're deficient, others disagree. For example, one study8,9 found that for every 10% increase in body-mass index, there's a 4.2% reduction in blood levels of vitamin D. According to the authors of that particular study, obesity may in fact be a causal factor in the development of vitamin D deficiency.10 Vitamin D Also Improves Colorectal Cancer OutcomesA scientific review11 published in the September 2020 issue of the British Journal of Cancer noted that having low vitamin D is associated with poor colorectal cancer survival. To assess whether vitamin D supplementation might improve survival in these patients, they reviewed the findings of seven trials, three of which included patients diagnosed with colorectal cancer from the outset and four population trials that reported survival in incident cases. Overall, the meta-analysis found supplementation resulted in a 30% reduction in adverse colorectal cancer outcomes. Vitamin D also improved outcomes among patients already diagnosed with colorectal cancer. According to the authors:12
Low Vitamin D Linked to Increased Cancer IncidenceAnother review and meta-analysis,13 this one published in November 2019 in Bioscience Reports, looked at vitamin D supplementation on cancer incidence and mortality in general. Ten randomized controlled trials with a pool of 81,362 participants were included in the analysis. While the incidence rate of cancer was very similar between the vitamin D intervention group and the placebo control group (9.16% versus 9.29%), the risk reduction in mortality was deemed "significant." As reported by the authors:
Vitamin D Protects Against Breast CancerSeveral studies have highlighted the benefit of vitamin D for breast cancer. For example, an analysis14 by GrassrootsHealth published June 2018 in PLOS ONE showed women with a vitamin D level at or above 60 ng/mL (150 nmol/L) had an 82% lower risk of breast cancer compared to those with levels below 20 ng/mL (50 nmol/L). An earlier study,15,16 which looked at women in the U.K., found having a vitamin D level above 60 ng/mL resulted in an 83% lower breast cancer risk, which is nearly identical to GrassrootsHealth's 2018 analysis. One of the more recent meta-analyses17,18 looking at breast cancer was published December 28, 2019, in the journal Aging. Here, they reviewed 70 observational studies, finding that for each 2 ng/mL (5 nmol/L) increase in vitamin D level there was a corresponding 6% decrease in breast cancer incidence. Overall, this translates into a 71% reduced risk when you increase your vitamin D level from 20 ng/mL to 60 ng/mL. The following graph, created by GrassrootsHealth,19 illustrates the dose response between vitamin D levels and breast cancer risk found in this study. 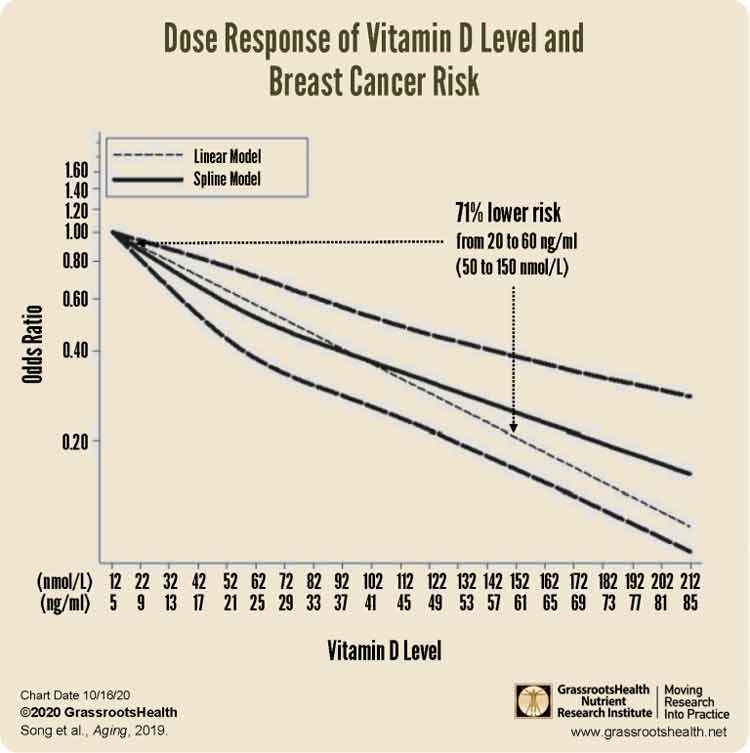 GrassrootsHealth's 2018 analysis in PLOS ONE also analyzed this dose relationship.20 To do that, they looked at the percentage of breast cancer-free participants in various vitamin D groups, from deficient (below 20 ng/mL) to optimal (at or above 60 ng/mL), over time (four years). As you might expect, the higher the blood level of vitamin D, the lower the incidence of breast cancer. The graph below illustrates this dose-related protection. At four years, the percentage of women who had been diagnosed with breast cancer in the 60 ng/mL group was 78% lower than among those with blood levels below 20 ng/mL. 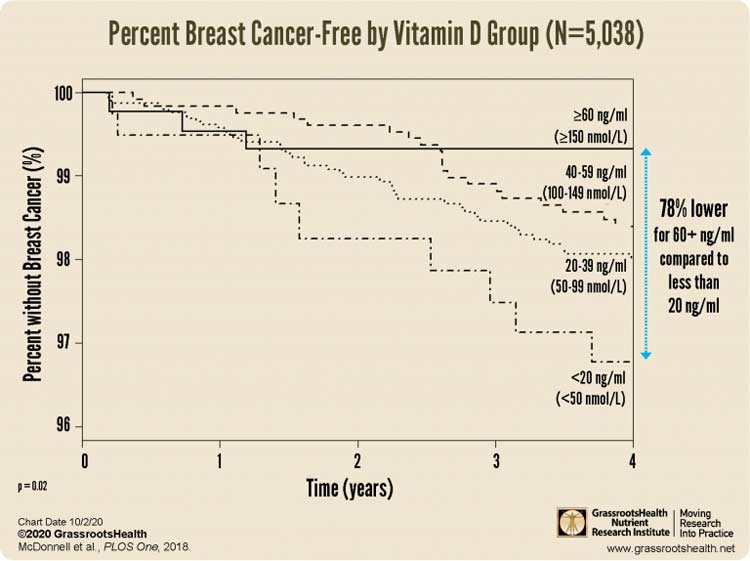 How to Optimize Your Vitamin D LevelIf you live in the northern hemisphere, which is currently heading toward winter, now is the time to check your vitamin D level and start taking action to raise it if you're below 40 ng/mL (100 nmol/L). As you can see from the studies above, a vitamin D level of 60 ng/mL (150 nmol/L) or higher is recommended if you want to protect against cancer. An easy and cost-effective way of measuring your vitamin D level is to order GrassrootsHealth’s vitamin D testing kit. Once you know your current vitamin D level, use the GrassrootsHealth vitamin D calculator21 to determine how much vitamin D you might need to reach your target level. To optimize vitamin D absorption and utilization, be sure to take your vitamin D with vitamin K2 and magnesium. Lastly, remember to retest in three to four months to make sure you’ve reached your target level. If you have, then you know you’re taking the correct dosage. If you’re still low (or have reached a level above 80 ng/mL), you’ll need to adjust your dosage accordingly and retest again in another three to four months. from http://articles.mercola.com/sites/articles/archive/2021/10/26/vitamin-d-to-prevent-tumor-death.aspx In the video above retired nurse lecturer John Campbell, Ph.D., reports on a comparative analysis of molnurpirivir and ivermectin published in the Austin Journal of Pharmacology and Therapeutics.1 The first is Merck's new antiviral drug and the second is the much vilified and maligned2,3 antiparasitic drug used in humans since 19874 and approved for human use in the U.S. in 1996.5,6 Campbell compares the efficacy, safety and cost using available data for ivermectin published in peer reviewed studies and the first interim data for molnupiravir published by Merck. Molnupiravir, also known as EIDD-2801/MK-44827 has data published as early as October 2019 that showed it was a clinical candidate for monotherapy in influenza viruses.8 And yet, Merck's investigation into the oral antiviral medication against SARS-CoV-2 was not logged with Clinical Trials until October 5, 2020.9 While Gilead raced to release remdesivir, posting their first clinical trial February 5, 2020,10 Merck appeared to be slow off the mark. Gilead suspended or terminated the early trials for remdesivir. The reasons given included:
The advantage molnupiravir has over remdesivir is that it is administered orally and can be used for early treatment in an outpatient setting. However, as we review the comparison between the drugs, it's important to remember that the early data on molnupiravir has been published in a press release.13 How Do Ivermectin and Molnupiravir Stack Up Against COVID-19?In the video Campbell reviews a paper published in the Austin Journal of Pharmacology and Therapeutics14 that was a chemical comparison of the pharmacological effects of molnupiravir and ivermectin. Looking at the two ways science uses to develop new treatments when a new condition arises,15 Campbell explains the first is to create a new drug and the second is to repurpose medications used for other conditions. For example, aspirin originally was used to treat fever. Once it became evident that it was also effective against pain, doctors began recommending it to relieve headaches and other minor aches and pains. Subsequently, it was found that aspirin was an effective antiplatelet, as well, and this function was added to the known uses for aspirin. According to the paper,16 Ivermectin is the "most studied, 'repurposed' medication globally, in randomized clinical trials, retrospective studies and meta-analysis." Ivermectin is an FDA-approved, broad spectrum antiparasitic17 with known anti-inflammatory properties.18 As Campbell reviews, an in vitro study19 demonstrated that a single treatment with ivermectin effectively reduced viral load 5,000 times in 48 hours in cell culture. By comparison, Merck claims molnupiravir is a broad-spectrum antiviral that is active against the Gamma, Delta and Mu SARS-CoV-2 variants.20 The data in the comparison paper show molnupiravir is more potent in-vitro than ivermectin,21 which means it needs less drug to work with a lower tissue concentration.22 The amount of time the maximum drug dose is found in the serum is one to 1.75 hours for molnupiravir and four to six hours for ivermectin. Interestingly, the half-life for Merck's drug is seven hours and the half-life for ivermectin is 81 to 91 hours. This is the amount of time it takes for your body to reduce the active ingredients in the drug by half. Campbell also reviews the following factors: • Safety -- No matter how well a drug works, if it's not safe for use, it cannot be effective. Offering some examples of how ivermectin's safety compares to other drugs, according to Campbell23 the global database of the World Health Organization, VigiBase, recorded 5,593 adverse events from ivermectin after 3.7 billion doses were administered to humans. For comparison, VigiBase recorded 136,222 adverse events for amoxicillin and 165,479 for ibuprofen. At this time there is no VigiBase data available for molnupiravir, so no comparisons can be made for that drug yet. To take the example one step further, an outside look at acetaminophen adverse events shows that this drug (aka Tylenol) is many times more dangerous than ivermectin. In the U.S. alone24 the National Institutes of Health's STATPearls manual reports that there are 2,600 hospitalizations, 56,000 emergency room visits and 500 deaths each year for acetaminophen overdoses as of July 2021. And, the drug is the second leading cause of liver transplantation worldwide and the leading cause of transplantation in the U.S. • Efficacy -- According to interim data from Merck,25 molnupiravir reduced hospitalizations or deaths by 50% in 385 participants who had at least one risk factor associated with poor disease outcome. A meta-analysis of 15 trials26 that included 2,438 participants demonstrated that ivermectin could reduce the risk of death by 62%. According to an ongoing collection from published data,27 across all studies ivermectin is 86% effective prophylactically, 66% effective in early treatment and 36% effective in late treatment. By comparison, a Cochrane review of the literature28 that Campbell references in the video found the data did not determine if ivermectin leads to more or less infections, worsened or improved infection, or increased or decreased unwanted events. • Cost -- According to a Forbes report,29 the raw material for the active pharmaceutical ingredients in molnupiravir costs about $2.50 per treatment. The cost of manufacturing the product would be $20, which is 35 times less than the price set by Merck of $700 per treatment. Additionally, Forbes reports that initially the drug will be purchased using federal funds. According to the treatment protocol by the FLCCC,30 ivermectin is dosed at 0.4 to 0.6 mg/kg of body weight per dose once daily for five days. For an average person 160 pounds (72.5 kg), the dose is 29 mg to 43.5 mg per day for five days. The average cost for 30 tablets of 3 mg of ivermectin in the U.S. can run as high as $108 or as little as $29.72 with a drug discount program — a fraction of molnupiravir's prices.31 Peer Reviewed Study May Answer Molnupiravir QuestionsAs I mentioned, according to the data released by Merck, molnupiravir reduced the risk of hospitalization or death by 50% as compared to the placebo group.32 According to the numbers in their study, 28 people in the intervention group died or were hospitalized by Day 29 while 53 in the placebo treated group were hospitalized or died. Merck did not identify the placebo in either their press release33 or in the Clinical Trials data.34 Dr. James Lyons-Weiler also evaluated the results of the trial and asked some very pertinent questions, such as:35 • Why were patients taking a placebo allowed to die?
• Why are the number of participants low? -- When the study was first listed on Clinical Trials36 the team initially anticipated 1,450 patients in a parallel phase 2/3 randomized, placebo-controlled study. This changed May 25, 2021, to 1,850 participants anticipated.37 At the completion of the study when they were no longer recruiting participants, they reported data on 762 participants in the press release38 from 173 locations. What happened to the data from the rest of the participants? • Why was the second study for hospitalized patients terminated? -- A second study39 was ongoing during the same time period for hospitalized patients, having started October 5, 2020, and last updated September 9, 2021. They anticipated enrolling 1,300 patients but terminated the study for "business reasons" after enrolling 304. What happened to cause the company to close this arm of the study after enrolling so few patients and what happened to the data? Lyons-Weiler is a senior research scientist at the University of Pittsburgh.40 He also listed the numerous exclusion criteria for participants in the study and went on to write:41
CBS News42 reports that Merck has asked U.S. regulators for emergency use authorization for the drug against COVID-19. The decision could come in just a few weeks and "The FDA will scrutinize company data on the safety and effectiveness of the drug, molnupiravir, before rendering a decision." It is hoped the FDA has access to all the data. Do We Really Need a Vaccine and a Treatment?Although Campbell adamantly defends the need for both a vaccine and treatment,43 he also points to diseases such as the bubonic plague for which we have adequate treatment but do not have a vaccine,44 even for areas of the world where it may have greater incidence.45 Campbell also believes that if there is a good quality antiviral medication, there would be less of an impact from COVID in countries where the vaccine rollout is patchy. And yet, data show that the number of confirmed cases of COVID in countries where much of the population is unvaccinated is not higher than in countries where nearly 100% have been given the jab. For example, as of October 13, 2021, according to the CNN COVID-19 vaccination tracker46 and the Johns Hopkins Coronavirus Resource Center:47
In the past, according to the CDC's definition, a vaccination program used a product that "stimulates a person's immune system to a specific disease, protecting the person from that disease."49 But today, CDC's new definition says vaccines are only meant to "stimulate the body's immune response against diseases."50 You'll note that the new definition says a vaccine isn't responsible for stimulating the immune system or protecting against any specific illness. According to COVID-19 statistics from the CDC,51 people over 65 carry the greatest burden of mortality. In 2020 this population accounted for 80.7% of deaths and thus far in 2021 this age range accounts for 71.2% of deaths in the U.S. However, these percentages are highly skewed since, to date, large populations of people are not offered or treated with successful protocols. This begs the question: How high has the CDC and FDA allowed the death rate to go by suppressing effective treatments that are readily available and economical? Prophylaxis and Early Treatment May Not Require MedicationWhile ivermectin has demonstrated it is a useful strategy, it's not my primary recommendation. You don't necessarily need prescribed medication to help prevent, and in the early treatment of, COVID-19. I believe your best option to fighting the onset of any disease is to optimize your vitamin D level, as your body requires this for a wide variety of functions, including a healthy immune response.52,53 Then, for early treatment, or after you've been exposed to someone with COVID, I recommend using nebulized hydrogen peroxide treatment.54 This treatment is inexpensive, highly effective, can easily be done at home and is completely harmless when you're using the low (0.04% to 0.1%) peroxide concentration recommended. In the video below I demonstrate how to make a low concentration of hydrogen peroxide at home and how to use your nebulizer. You'll find my interviews with Dr. Thomas Levy55 and Dr. David Brownstein56 about this treatment on Bitchute. from http://articles.mercola.com/sites/articles/archive/2021/10/25/ivermectin-vs-molnupiravir.aspx This article was previously published January 25, 2021, and has been updated with new information. Knowledge is power. So is ownership, including land ownership. Did you know that Bill Gates is America's top farmland investor? This short video reveals many of the global strategies Gates has been using to influence your health and the food supply. Through his founding of the second-largest technological company in the world,1 Gates has developed financial and influential relationships with powerful organizations responsible for many global decisions that affect your life. Subtly, and sometimes not so subtly, his movements have grown a massive financial empire and expanded his ability to create change to support his goals. Gates is also a supporter of the "Great Reset" that promises "social cohesion, fairness, inclusion and equality,"2 while allowing elite billionaires to practice strategies that grew his and other billionaires' wealth by 26% during the pandemic in 2020.3 In other words, while supporting Marxist principles to spread the wealth — so by 2030 you can say, "I Own Nothing, Have No Privacy and Life Has Never Been Better"4 — he is enjoying the fruits of his labor by accumulating more wealth and property, a decidedly different approach to the Great Reset he promotes. Put plainly, the political and ideological foundations of Marxism have once again surfaced, and in some arenas, are celebrated. However, it's vital to remember that unlike Walgreens' advertising campaign featuring a picture-perfect town of "Perfect,"5 Marxist philosophy has created tyranny and was responsible for the deaths of more than 100 million people in the last century, as aptly described by James Bovard in USA Today.6 History is studied and shared so the mistakes of the past are not repeated. However, it’s evident there are many who have forgotten, or never learned, what resulted behind the Iron Curtain from implementing the socialist principles which now underpin The Great Reset. The Great Reset or Fourth Industrial Revolution has strong supporters among wealthy technocrats who will not redistribute their own wealth, but will only continue to grow their financial empires as the rest of the world suffers. Indeed, 2020 has only been a taste of what could come as more people lose their jobs and financial security, while those controlling the event become wealthier. Bill Gates Is Now the Biggest Farmland OwnerThe Land Report announced that multibillionaire Bill Gates currently holds the title as America's biggest private farmland owner. He owns 242,000 acres, nearly 52,000 more than the next largest farmland owner.7 To put this in perspective, 52,000 is equal to 39,325 football fields, including the end zones.8 His farmland (approximately 378.125 square miles) would rank in total land mass as the eighth largest city in the U.S. in 2010.9 It was Eric O'Keefe from the Land Report10 who ferreted out the story after reading that 14,500 acres of choice farmland in Benton County, Washington, had been sold for $171 million, or nearly $12,000 per acre. O'Keefe describes the area as "some of the richest farmland in the Lower 48," that "savvy investors have been plowing millions of dollars into."11 Although the seller was listed as John Hancock Life Insurance, the buyer was reported as a limited liability company from Louisiana. Digging deeper and engaging their research team, he discovered the paper trail led to a company managed by Michael Larson, manager of the Gates' personal portfolio and much of the Bill and Melinda Gates Foundation for the last 25 years. Larson primarily uses Cascade Investment LLC as the entity through which he manages their personal portfolio. O'Keefe details the sequence in which the land changed hands over 10 years. The largest single block of farmland was quietly acquired by Cascade in 2017, one year after it was purchased by a Canadian firm.12 The sale was revealed in the Canadian firm's quarterly statement, in which they reported offloading $520 million in farmland offered in a single block. An investigative journalist ultimately found the half-billion-dollar sale led to Cascade Investment LLC. Gates Is Not the Largest Individual LandownerGates owns a substantial amount of land, for a total of 268,894 acres if you count his transitional and recreational properties. But, he's not the only billionaire who tops the Land Report list. Stewart and Lynda Resnick, co-founders of Wonderful Company, come in at No. 2, owning 190,000 acres. They use their farmland to support their food products, such as Wonderful Pistachios and Wonderful Halos Mandarin oranges.13 Gates also is not the largest individual landowner overall, as that spot goes to John Malone, chairman of the board at Liberty Media Corporation and former chief executive officer for Tele-Communications Inc.14 Malone owns 2.2 million acres of forest and ranch land; media Mogul Ted Turner owns 2 million across eight states.15 Amazon CEO Jeff Bezos is also heavily invested in land, coming in the 25th spot at 420,000 acres located mostly in Texas.16 The remaining list is filled with recognizable names, including the King Ranch, Ford family and the Kennedy Memorial Foundation.17 In addition to farmland, Cascade Investment has purchased 24,800 acres of transitional property west of Phoenix, which is poised for city expansion projected to include: “up to 80,000 homes; 3,800 acres of industrial, office and retail space; 3,400 acres of open space; and 470 acres for public schools."18 Cascade also bought 1,234 recreational acres, making the land Gates owns through just Cascade Investment LLC at 268,984 acres. Separate from the Gates’ personal holdings is the Bill and Melinda Gates Foundation, which has no ties to Cascade, but does have a farmland initiative called Gates Ag One, which19
What Is the Leading Harvest Standard?Although Cascade Investment has declined to make any comment on the quiet transactions through the Canadian company, they have come out in support of sustainable farming. One of the entities owned by Cascade, Cottonwood Ag Management, is an initial member of Leading Harvest, a nonprofit organization formed to advance:20
As O'Keefe describes it, the goal is to create a "sustainability standard that can be implemented across the greatest swath of agricultural acreage."21 Yet, while this goal is commendable, they remain words on paper without a substantive foundation. In other words, according to the organization, they do not offer farmers guidance to achieve the goal, only the formation of a certification program to audit the farmers' results.22 In their publication, they describe the program:23
In other words, instead of guidance and standards for how the farmer achieves sustainability and protects the future of farming, they created a certification for farmers to demonstrate their participation in developing practices where the end result meets their standard — do the ends justify the means? Gates Seeking Sustainable Energy in All the Wrong PlacesGates has been calling for sustainable energy and a reduction of carbon emissions for over a decade.24 At one point in a 2010 TED talk, he questioned if we need another Manhattan Project to discover a renewable and safe energy source. If you don't remember, the Manhattan Project was the code name given to an operation aimed at discovering a functional nuclear weapon,25 that resulted in a bomb being dropped on Hiroshima, Japan. When asked how he would deal with climate change skeptics, he said:26
Gates spoke about climate change and the technological advancements that may be necessary in an interview with a journalist from The Atlantic in 2015. The journalist recorded this response:27
Gates Calls Plant-Based and Lab-Grown Meat SustainableWhile Gates may not think highly of the government or entrepreneurs, he does believe that plant-based and lab-grown meat alternatives are healthy and sustainable. Historically, some of the decisions from the Gates Foundation haven’t been focused on the environment but, rather, cloaked in rhetoric that appears environmentally friendly. For example, despite a lack of consensus on GMO safety,28 in 2010 the Gates Foundation aligned itself with Monsanto and Cargill. They invested nearly $23 million in 500,000 Monsanto shares. Subsequently, a South African watchdog group discovered the Gates Foundation had also invested $10 million in Cargill to "develop the soya value chain,"29 which The Guardian wrote probably meant the "big time introduction of GM soy in southern Africa."30 In 2010, The Guardian also reported that Gates had funded research to develop machines that would spray seawater into the clouds with the goal of increasing the ability to reflect sunlight into space, and therefore reduce global warming. The move triggered a call for a global ban on geoengineering experiments from the ETC Group and a comment from co-executive director Jim Thomas:31
Not to be deterred by naysayers, eight years later in 2018 Gates agreed to help fund experiments for Harvard scientists, who proposed to spray the stratosphere with calcium chloride to help slow the Earth's warming.32 In keeping with past decisions, Gates also supports plant-based and lab-grown meat alternatives,33,34 which are riddled with patented chemicals and genetically engineered ingredients. Seth Itzkan from Soil4Climate, characterizes one fake-meat product this way:35
Presumably, his support of chemical food, reminiscent of the DuPont slogan "Better things for better living through chemistry,"36 is to reduce carbon emissions. However, as has been documented and covered in other articles I’ve written, regenerative farming practices are better for the land, the animals and your health. Your Health Depends on Whole FoodConvinced that their method of producing chemical-based food reduces the carbon footprint, Impossible Foods hired Quantis to give them scientific evidence.37 According to the executive summary published on their website, their product reduces the environmental impact between 87% and 96% in the categories Quantis studied, including global warming potential, land occupation and water consumption. However, Quantis compared fake meat production against CAFOs, which are notoriously destructive. On the other hand, White Oak Pastures in Bluffton, Georgia, practices true sustainable, regenerative farming and produces high-quality, grass fed products. White Oak Pastures commissioned the same analysis, by the same company, which showed they had a net total emission in the negative numbers.38 It's also worth noting that the Impossible Burger is made from GMO soy containing glyphosate. Your health and longevity are dependent on providing your body with necessary nutrients from whole food. It's simply impossible to be sustained by synthetic chemicals, toxic GMO grains contaminated with pesticides and fake meat. Regenerative farming practices can provide whole food and can have a positive impact on the environment. Imagine the powerful influence Gates could have on the environment and the country if he would move his massive acreage into regenerative farming practices. This could raise the quality of food the land produces and demonstrate sustainable practices that can be followed around the world. Instead, it appears that financial motivations are helping to drive environmental decisions to support his personal goals. As I’ve discussed in other articles, the movement to develop fake food is lucrative. However, you can protect your health and your future by starting with a few simple guidelines that include always choosing organic foods, buying from local farmers and never eating processed foods of any sort. from http://articles.mercola.com/sites/articles/archive/2021/10/25/bill-gates-biggest-private-farmland-owner.aspx In early September 2021, Oklahoma’s KFOR news ran a falsified story about emergency rooms being overrun with patients who had overdosed on horse ivermectin.1 Other mainstream media followed suit — all incorrectly referring to ivermectin as a dangerous veterinary drug. In the real world, ivermectin is a human drug that has been safely used by 3.7 billion people since the early 1990s.2 In 2016, three scientists received the Nobel Prize in physiology or medicine for their discovery of ivermectin against parasitic infections in humans.3 It’s also on the World Health Organization’s list of essential medicines.4 There’s absolutely no reason whatsoever to disparage ivermectin as a “horse dewormer” that only a loony person would consider taking. Yet that’s what mainstream media have done, virtually without exception. When comedian and podcast host Joe Rogan revealed5 he’d treated his bout of COVID-19 with ivermectin and other remedies — fully recovering within three days — NPR reported Rogan had taken “ivermectin, a deworming veterinary drug that is formulated for use in cows and horses,” adding that “the Food and Drug Administration is urging people to stop ingesting” the medication, saying animal doses of the drug can cause nausea, vomiting and in some cases severe hepatitis.6 Sanjay Gupta Admits CNN LiedCNN, among many others, also reported on Rogan’s use of “horse dewormer.” In mid-October 2021, Rogan interviewed CNN medical correspondent Dr. Sanjay Gupta, grilling him on why CNN would outright lie about his use of ivermectin.
Gupta finally relents and agrees that ivermectin should not be called horse dewormer. When asked, “Does it bother you that the news network you work for out and out lied about me taking horse dewormer?” Gupta replied, “They shouldn’t have said that.” When asked why they would lie about such an important medical issue, Gupta replied “I don’t know.” Gupta also admits he never asked why they did it, even though he’s their top medical correspondent. FDA Attacks IvermectinWhile CNN and mainstream media are certainly at fault for spreading disinformation here, they got the idea from a supposedly reputable source — the FDA. In an August 21, 2021, tweet,7 the FDA linked to an agency article warning against the use of ivermectin, saying “You are not a horse. You are not a cow. Seriously, y’all. Stop it.” This blatantly misleading post seeded the lie that then spread across mainstream media. In an article posted on RESCUE with Michael Capuzzo substack, two independent investigative health journalists, Mary Beth Pfeiffer and Linda Bonvie, detail how the FDA’s anti-ivermectin campaign began:8
The now infamous tweet was born out of a single sentence in a Mississippi poison control health alert, which stated that “At least 70% of the recent calls have been related to ingestion of livestock or animal formulations of ivermectin purchased at livestock supply centers.” The problem? That wasn’t accurate either. Much Ado About NothingAs it turns out, the real percentage of recent calls to poison control related to veterinary ivermectin was 2%, not 70%. In an October 5, 2021, correction, the Mississippi health department clarified that it wasn’t 70% of all poison control calls that involved veterinary ivermectin, it was 70% of all ivermectin-related calls.9 In absolute numbers, there were six such calls, and four of those calls actually related to livestock accidentally receiving the drug. Investigation by Pfeiffer and Bonvie also revealed that between July 31 and August 22, 2021, 40%, 10 of 24 ivermectin-related calls to the Mississippi poison control center were mere requests for information, which is a common occurrence.
Ivermectin Is Safe; Remdesivir, Not so MuchAccording to VigiAccess, the World Health Organization’s drug tracker, a total of 20 deaths have been linked to ivermectin since 1992.13 Compare that safety profile to remdesivir, the primary drug used by hospitals across the U.S. against COVID-19. Since the spring of 2020, VigiAccess has received 7,491 adverse events in all attributed to remdesivir, including 560 deaths, 550 serious cardiac disorders and 475 acute kidney injuries.14 The question is why remdesivir is being used at all, with the World Health Organization recommending15 against it and a new Lancet study16 finding “no clinical benefit.” Could it be that Fauci is involved with the fraud? Pfeiffer and Bonvie write.17,18
State AG Calls Out Medical Establishment for MisinformationIn better news, in early October 2021, the Nebraska Department of Health asked Nebraska Attorney General Doug Peterson to issue a legal opinion on the off-label use of ivermectin and hydroxychloroquine for COVID-19. October 15, 2021, Peterson issued a legal opinion20,21 stating health care providers can legally prescribe these medications for off-label use for the treatment of COVID, provided they have informed consent from the patient.22 The only causes for disciplinary action are failure to obtain informed consent, deception and/or prescribing excessively high doses. Peterson concluded that, based on the available evidence, hydroxychloroquine and ivermectin “might work for some people.” He highlighted studies demonstrating the safety and benefits of these drugs against COVID-19, as well as the shocking scientific fraud that led to worldwide shunning of hydroxychloroquine, and the cherry-picking and exclusion of data in studies that are critical of ivermectin. He also pointed out how illogical it is to discourage early treatment.
Peterson also called out the FDA and Dr. Anthony Fauci on their hypocrisy, detailing how the FDA and National Institutes of Health seeded confusion by issuing contradictory guidance. The NIH has taken a neutral position to ivermectin, which Peterson “clearly signaled that physicians should use their discretion in deciding whether to treat COVID-19 patients with ivermectin.” NIH officials, however, have ignored the agency’s official position. At the end of August 2021, Fauci “went on CNN and announced that ‘there is no clinical evidence’ that ivermectin works for the prevention or treatment of COVID-19,’ and that ‘there is no evidence whatsoever’ that it works,” Peterson writes, adding:
AG Blames FDA for Seeding ConfusionPeterson goes on to review the FDA’s behavior with respect to ivermectin:
Peterson also highlights the fact that while the FDA claims ivermectin “is not an antiviral (a drug for treating viruses),” on another FDA webpage they list a study in Antiviral Research that “identified ivermectin as a medicine ‘previously shown to have broad-spectrum antiviral activity.”
He also points out that while the FDA now claims off-label use of drugs “can be very dangerous,” and that this is why they don’t recommend ivermectin for COVID, doctors routinely use drugs off-label, and ivermectin has a well-established safety record. So, “it is inconsistent for the FDA to imply that ivermectin is dangerous when used to treat COVID-19 while the agency continues to approve remdesivir despite its spottier safety record,” Peterson writes. AG Puts Professional Associations Under the MicroscopePeterson also questioned the stance of professional associations such as The American Medical Association, American Pharmacists Association and American Society of Health-System Pharmacists, which in September 2021 issuing a joint statement25 opposing the use of ivermectin to prevent or treat COVID outside of clinical trials. Their statement, Peterson points out, relied on the FDA’s and CDC’s “suspect positions,” and a statement by Merck, in which they opposed the use of the drug due to a “concerning lack of safety data in the majority of studies.”
Another excellent article26 detailing the FDA’s questionable actions, and Merck’s incentives to disparage their old drug, ivermectin, was published by the American Institute for Economic Research.
Early Treatment Is CrucialThere’s no doubt that many have died unnecessarily due to our health authorities’ incomprehensible decision to discourage all prevention and early treatment of COVID-19. As noted by many doctors, early treatment is absolutely crucial for preventing hospitalization, death and long-term side effects of the infection. There are several proven protocols to choose from at this point, including the following. Whichever treatment protocol you use, make sure you begin treatment as soon as possible, ideally at first onset of symptoms.
from http://articles.mercola.com/sites/articles/archive/2021/10/25/fda-attacks-ivermectin.aspx |
Nia Pure NatureThe Provider of premium Quality Health Products To Live Better Lives Archives
March 2022
Categories |
 RSS Feed
RSS Feed
